Selçuk Candansayar: "Bilgisayar oyunu oynadı diye olmaz. Cinsel yönelimi farklı diye olmaz. Azınlık diye olmaz. Zengin diye değil, fakir diye değil, laik diye değil, laik değil diye değil. Her çocuk olabilir. Hiçbir öngörücüsü yok.
Tanımlanmış 3 tane şey var. Dışlanmışlık-yalnızlık, ırkçılığa varan üstünlükçülük duyguları ve kadın düşmanlığı. Çünkü saldırıların %90'ında failler erkek."
Tıp fakültelerindeki öğretim üyelerinin ve sağlık çalışanlarının özlük hakları düşük, çalışma koşulları ağır. Üniversite hastanelerine ayrılan kaynak yetersiz.
Sağlık sisteminin göz bebeği olan üniversite hastaneleri desteklenmelidir.
Breaking news = disappointing facts. 🚨
Here are some facts (from the trial): and don’t miss point 4️⃣
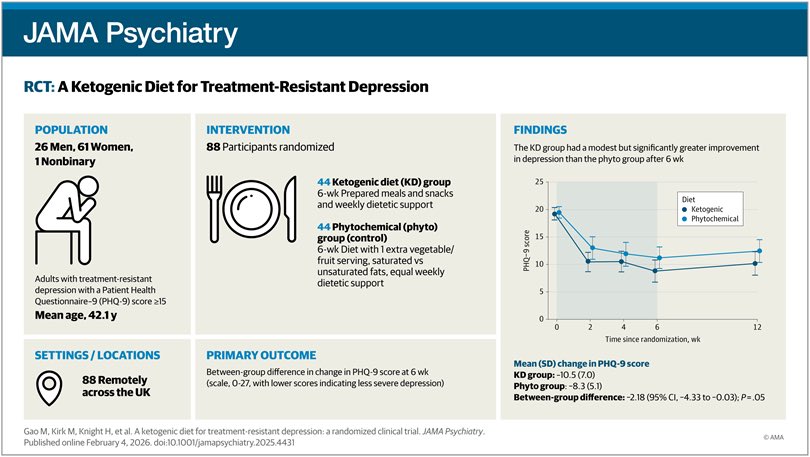
1️⃣This trial wasn’t keto only -
It was keto + weekly dietetic support + provided meals/snacks vs a control (“phyto”) diet + equal support (extra fruit/veg etc .. ).
2️⃣Both groups improved.
Mean PHQ-9 change at 6 weeks: KD −10.5 (SD 7.0) vs control −8.3 (SD 5.1).
“The absolute reduction in PHQ-9 score in the phyto group in our study was 8 points, suggesting that support and belief in the dietary program may have had an effect that was larger than any improvement specifically attributable to the KD.”
3️⃣Authors - “We aimed to detect a clinically meaningful 5-point difference in the PHQ-9 score”
Result 👉 at 6 weeks was ~2.2 points on a 0–27 scale ( less than what was considered clinically meaningful)
4️⃣Now the big one 👉is the ketosis the magic sauce ?
“Kendall τ-b correlations showed no significant association between ketone concentration and PHQ-9 score.
Participants with mean ketone levels of 1.5 mmol/L or greater (n = 23) had a mean (SD) change in PHQ-9 score of −8.4 (7.0)… By contrast, participants with mean ketone levels lower than 1.5 mmol/L (n = 20) showed a greater mean (SD) change in PHQ-9 score of −12.9 (6.3)…”
Wait a sec ! 👉So even within the KD arm, ketosis didn’t track antidepressant response ! if anything, the direction is the opposite. ( low ketones ; greater PHQ change )
So the question is does ketosis really have an antidepressant effect ? 🤔🤔
5️⃣CI - almost touch 0 (null) indicative of possibility of no change
6️⃣The effect didn’t hold at 12 weeks: −1.85 (95% CI −4.04 to 0.33), P = .10 → not significant.
7️⃣No separation on most patient-relevant secondary outcomes.
8️⃣Adherence drops off after trial 👉By week 12 (6 weeks after support ended) only 9% followed it nearly every day.
“Our trial was designed to assess efficacy by providing intensive support and supplementary food to maximize adherence to a KD, and we found that when all support stopped, few people continued the KD”
So is it breaking ? You be the judge .
Your brain on stimulants vs your brain on ADHD
There is more to what ADHD is than what stimulants do, and there is more to the clinical use of stimulants than the boundaries of ADHD
https://t.co/oynG47ECLw
@drjprogers@MeramCan@berkerduman@tompollak ve diğer çalışma arkadaşlarımızla birlikte multidisipliner bir ekiple (nöroloji, biyokimya, enfeksiyon hastalıkları, nükleer tıp, nöroradyoloji, romatoloji) @TheBJPsych açık erişimde yayımladığımız otoimmün katatoni yazımız için @almila_erol psikiyatri pratiğine yönelik önemli bir editöryal yazdı.
Değerli çalışma arkadaşlarımız ile @rifatilhan sorumluluğunda British J Psych açık erişimde yayımladığımız seronegatif otoimmün katatoni serisi hakkında @almila_erol tarafından yazılan editöryal, steroide yanıt veren otoimmün katatoni tablolarını ve psikiyatri pratiğine olası etkilerini ele alıyor.
https://t.co/slFxQ5VPnM
A real problem in psychiatry is when diagnosis becomes unfalsifiable. Labels like schizophrenia should be working hypotheses, not fixed identities. When every behavior is interpreted through the diagnosis, counterevidence disappears and misdiagnosis becomes entrenched.
Good practice means diagnoses are provisional, revisited and revised as new information emerges. When that does not happen, harm follows. The issue is not that psychiatric diagnosis cannot be questioned. It is that sometimes it is not questioned enough.
For clarity, lithium at lower than clinical doses doses is not typically toxic, and would not generally require blood tests, and has generally been found to be safe though not without risk for some (as noted, I don't advise people take lithium and certainly not without consulting with a qualified physician. There is also insufficient evidence for public health recommendations). A number of researchers in the field who I know personally do take a low dose of lithium daily, because they are at least personally convinced the risk-benefit ratio is favorable for themselves.
The risk for dementia is significantly reduced in patients taking lithium who have bipolar disorder, which has prompted researchers to wonder if it has broader benefit. Here's a recent meta-analysis https://t.co/UvXqdg4Pxb
Dietary and groundwater lithium exposure varies widely globally, with drinking water concentrations typically ranging from <1 to 30 μg/L in most regions, though some areas reach substantially higher levels. In the United States, groundwater lithium ranges from 0.9 to 161 μg/L (median 13.9 μg/L), while surface water ranges from <0.5 to 130 μg/L (median 3.9 μg/L).[1] Lithium in 56% of U.S. groundwater and 13% of surface water samples exceeded the non-regulatory Health-Based Screening Level of 10 μg/L.[1]
Potential Benefits
The most robust evidence supports mental health benefits. A meta-analysis of 14 studies including 94 million people found higher lithium concentrations in drinking water were associated with reduced suicide rates (β = -0.191).[2][3] Meta-analysis of two studies including 5 million people found fewer psychiatric hospital admissions (β = -0.413).[2] A Danish study of 73,731 individuals found higher lithium in drinking water was associated with lower dementia incidence.[4]
Dietary intake from food sources also contributes to total lithium exposure. Although lithium is not considered an essential nutrient, some evidence suggests a provisional recommended dietary allowance of 1.0 mg/day for a 70 kg adult may be beneficial.[5] Vegetables and drinking water are major sources of human lithium intake.[4][5] Portuguese natural mineral waters show highly variable lithium content, with some exceeding 1500 μg/L; consuming just 0.25 L/day of high-lithium mineral water (2220 μg/L) could provide up to 50% of the proposed 1 mg/day requirement.[6]
Potential Risks
Recent evidence has raised concerns about developmental and other health outcomes. A Danish population-based study found higher maternal exposure to lithium in drinking water (range 0.6-30.7 μg/L) during pregnancy was associated with increased risk of autism spectrum disorder in offspring.[7] A 2025 large-scale U.S. analysis found associations between lithium in groundwater and cancer risk, though concentrations were substantially lower than therapeutic levels.[8]
Conventional drinking water treatment processes do not remove lithium, as demonstrated by nearly identical concentrations in paired source water and treated drinking water samples.[1] This raises considerations for direct and indirect potable reuse, as wastewater effluents contain lithium at 0.8-98.2 μg/L (median 9.9 μg/L).[1]
Geographic Variation and Exposure Modeling
Lithium concentrations show substantial geographic variation related to geology, climate, and water sources. Concentrations are highest in arid regions and older groundwater, particularly in unconsolidated clastic aquifers and sandstones.[9] A nationwide U.S. model predicts lithium probability in four concentration classifications (≤4, >4 to ≤10, >10 to ≤30, and >30 μg/L) with 47-65% accuracy, using predictor variables including precipitation, well depth, and soil geochemistry.[10]
Key Study Links
1. Lithium Occurrence in Drinking Water Sources of the United States. Chemosphere. 2022. Sharma N, Westerhoff P, Zeng C. https://t.co/IZgIsH1M9N
2. The Association Between Lithium in Drinking Water and Neuropsychiatric Outcomes: A Systematic Review and Meta-Analysis From Across 2678 Regions Containing 113 Million People.
The Australian and New Zealand Journal of Psychiatry. 2021. Eyre-Watt B, Mahendran E, Suetani S, et al. https://t.co/9xisCClndb
3. Association Between Naturally Occurring Lithium in Drinking Water and Suicide Rates: Systematic Review and Meta-Analysis of Ecological Studies.
The British Journal of Psychiatry : The Journal of Mental Science. 2020. Memon A, Rogers I, Fitzsimmons SMDD, et al. https://t.co/1OPDsVI2mN
4. Association of Lithium in Drinking Water With the Incidence of Dementia.
JAMA Psychiatry. 2017. Kessing LV, Gerds TA, Knudsen NN, et al. https://t.co/Lf0VEG0g5s
5. Lithium: Perspectives of Nutritional Beneficence, Dietary Intake, Biogeochemistry, and Biofortification of Vegetables and Mushrooms.
The Science of the Total Environment. 2021. Naeem A, Aslam M, Saifullah, Mühling KH. https://t.co/QqqzBAXFx6
6. Lithium in Portuguese Bottled Natural Mineral Waters-Potential for Health Benefits?.
International Journal of Environmental Research and Public Health. 2020. Neves MO, Marques J, Eggenkamp HGM. https://t.co/lIxfhlhzZg
7. Association Between Estimated Geocoded Residential Maternal Exposure to Lithium in Drinking Water and Risk for Autism Spectrum Disorder in Offspring in Denmark. JAMA Pediatrics. 2023. Liew Z, Meng Q, Yan Q, et al. https://t.co/VTHAyrpuKT
8. Cancer Risk and Estimated Lithium Exposure in Drinking Groundwater in the US. JAMA Network Open. 2025. Luo J, Zheng L, Jin Z, et al https://t.co/YBhXpH6sG7
9. Lithium in Groundwater Used for Drinking-Water Supply in the United States.
The Science of the Total Environment. 2021. Lindsey BD, Belitz K, Cravotta CA, Toccalino PL, Dubrovsky NM. https://t.co/3sOdeCI1Du
10. Estimating Lithium Concentrations in Groundwater Used as Drinking Water for the Conterminous United States. Environmental Science & Technology. 2024. Lombard MA, Brown EE, Saftner DM, et al. https://t.co/9GoZUh9svw
Kanabis (esrar) kullanımının yasallaştığı yerlerde yeni şizofreni vakalarında 3 kata yakın artış bildirilmiş📌
Kanabis, psikozla nedensel ilişkisi kanıtlanmış bir madde.