"I’m sorry that I have no words of wisdom or inspiration. I get sad and scared too. I think maybe it’s part of the natural price of wanting to do this kind of work."
~David Foster Wallace
https://t.co/T2gIfa5TWh
When I applied to medical school in 1996, lots of people (attendings, residents, some family members) told me the profession was doomed because of HMOs, longer hours, and lower pay. It's been 30 years, and medicine is still in demand, with excellent job security. Don't let the current fatalists get you down. The world will always need doctors.
Every year, I share this video of French caretakers who take sand from Omaha Beach in Normandy, and scrub them into the letters to give them the gold coloring.
They do this for all 9,386 US soldiers who died.
France also gave us this land as American soil. #MemorialDayWeekend
This is one of the most out of touch takes I’ve ever heard from a fellow physician.
Read the room, Congressman.
Physicians are burning out because we are being crushed by administrative burden, loss of autonomy, declining reimbursement, corporate consolidation, insurance interference, and a system that treats doctors like disposable labor while demanding endless sacrifice.
Stop blaming physicians for refusing to tolerate an increasingly dysfunctional system. The problem is not that young doctors lack commitment. The problem is that medicine has become unsustainable.
Want to know the most valuable asset on a hospital’s campus or within an entire health system?
A physician’s signature.
The irony is that everyone knows it except the physician.
The way to attract more physicians to primary care is to reimburse PCPs fairly, not to give a bunch of upfront free stuff for everyone to devour. And yes, medical education is insanely expensive in this country, but that’s an entirely different topic.
On Memorial Day, we pay tribute to the brave men and women in uniform who gave their lives for this country that we love. It is a debt we can never fully repay, but we must never stop trying. I’ll always be grateful to our fallen heroes and their families, whose sacrifice reminds us of what it means to live for something greater than ourselves.
I honestly don't think med school debt has led to the death of independent physician practice.
When the hospital conglomerate can charge twice as much for the same clinic visit or procedure, or when they can play arbitrage games with drug discount programs that independent doctors don't get, or when they get massive tax exemptions, that leads to a financial imbalance which is impossible to rectify.
The independent physician practice is worth more to the large hospital conglomerate than it is to the independent physician. No amount of debt-free medical education will change that.
@neoavatara People always assume fixing the physician shortage means opening up the training pipeline.
How about we make the profession less miserable so people practice longer?
"Until death, all defeat is psychological." - Marcus Aurelius
Refuse everything that would lead most people to give up.
Refuse it.
Rise from the dead 1000 times.
Commit to never stay down & never give up.
Everything you want is on the other side of struggle.
Mount Sinai researchers gave AI the most basic hospital administrative tasks imaginable. Count the patients. Filter by age. Apply exclusion criteria. Simple table operations that any data analyst does daily.
The AI failed. On tables as small as 25 rows.
Not because it didn't understand the question. It understood perfectly. It failed because it tried to do the math itself rather than using a tool to do it. It made counting errors. It sounded confident. It was wrong.
Then they gave the models the ability to write and execute code. The same models that had failed went to near-perfect accuracy. Same question. Same data. Different architecture.
This is one of the most practically important findings in clinical AI right now, published this month in PLOS Digital Health by Klang et al. at Mount Sinai. Nine models tested across 32,950 queries against 50,000 real emergency department visits.
The results were consistent across every model tested. Direct prompting: poor accuracy that collapsed as tables got larger. Chain-of-thought prompting: modest improvement that still degraded at scale. Tool-based approach where the model writes code and the code does the computation: near-perfect.
The implication for healthcare is immediate. Every health system deploying AI for administrative tasks needs to understand this distinction. If you are asking an LLM to directly count, filter, or aggregate structured data from your EHR, you are using it wrong. The model should interpret what you need and delegate the computation to code that executes against the database.
This is the same principle showing up everywhere in clinical AI. The models that perform best are never used in isolation. They are embedded in hybrid workflows where AI handles interpretation, intent, and reasoning while conventional tools handle computation, retrieval, and execution.
How you use the model can matter more than which model you use. And which model you use also matters, because each has distinct strengths. The architecture and the capability are both variables. Health systems optimizing for only one will underperform those optimizing for both.
https://t.co/84d3b45aqx
This is my favorite study of the year.
What a waste of money. But keep telling physicians to see more patients every hour. Because that is working so well….
Winston Churchill fought his depression with bricks. He'd lay them for hours at his country home in Kent. He joined the bricklayers' union. And in 1921 he wrote about why it worked. It took psychology another 75 years to catch up.
He called his depression the "Black Dog." It followed him for decades. His method for fighting it back was as basic as it sounds: laying brick after brick, hour after hour.
Churchill spelled out his theory in a long essay for The Strand Magazine. People who think for a living, he wrote, can't fix a tired brain just by resting it. They have to use a different part of themselves. The part that moves the eyes and the hands. Woodworking, chemistry, bookbinding, bricklaying, painting. Anything that drags the body into a problem the mind can't solve by itself.
Modern psychology now calls this behavioral activation. It's one of the most-studied depression treatments out there. Depression sets a behavior trap. You feel bad, so you stop doing things, and doing less means less to feel good about. Feeling worse makes you do even less. The loop tightens until you can't breathe inside it.
Behavioral activation breaks the loop from the action side. You schedule the activity first, even when every part of you doesn't want to. Doing it produces small rewards: a wall gets straighter, a painting fills in, a messy room gets clean. Those small rewards slowly rewire the brain. Action comes first, and the feeling follows.
Researchers at the University of Washington put this to the test in 2006. They studied 241 adults with major depression and compared three treatments: behavioral activation, regular talk therapy, and antidepressants. For the people who were most severely depressed, behavioral activation matched the drugs. It beat the talk therapy. A 2014 review of more than 1,500 patients across 26 trials backed up the result.
Physical work like bricklaying does something extra on top of this. It crowds out rumination, the looping bad thoughts that grind people down during the worst stretches of depression. Bricklaying needs both hands and gives feedback brick by brick: each one is straight or crooked. After an hour you can see exactly how much wall you built. No room left for the mental chewing.
The line George Mack used in his post, "depression hates a moving target," is good poetry. The science behind it is sharper. Depression hates a brain that has somewhere else to be.
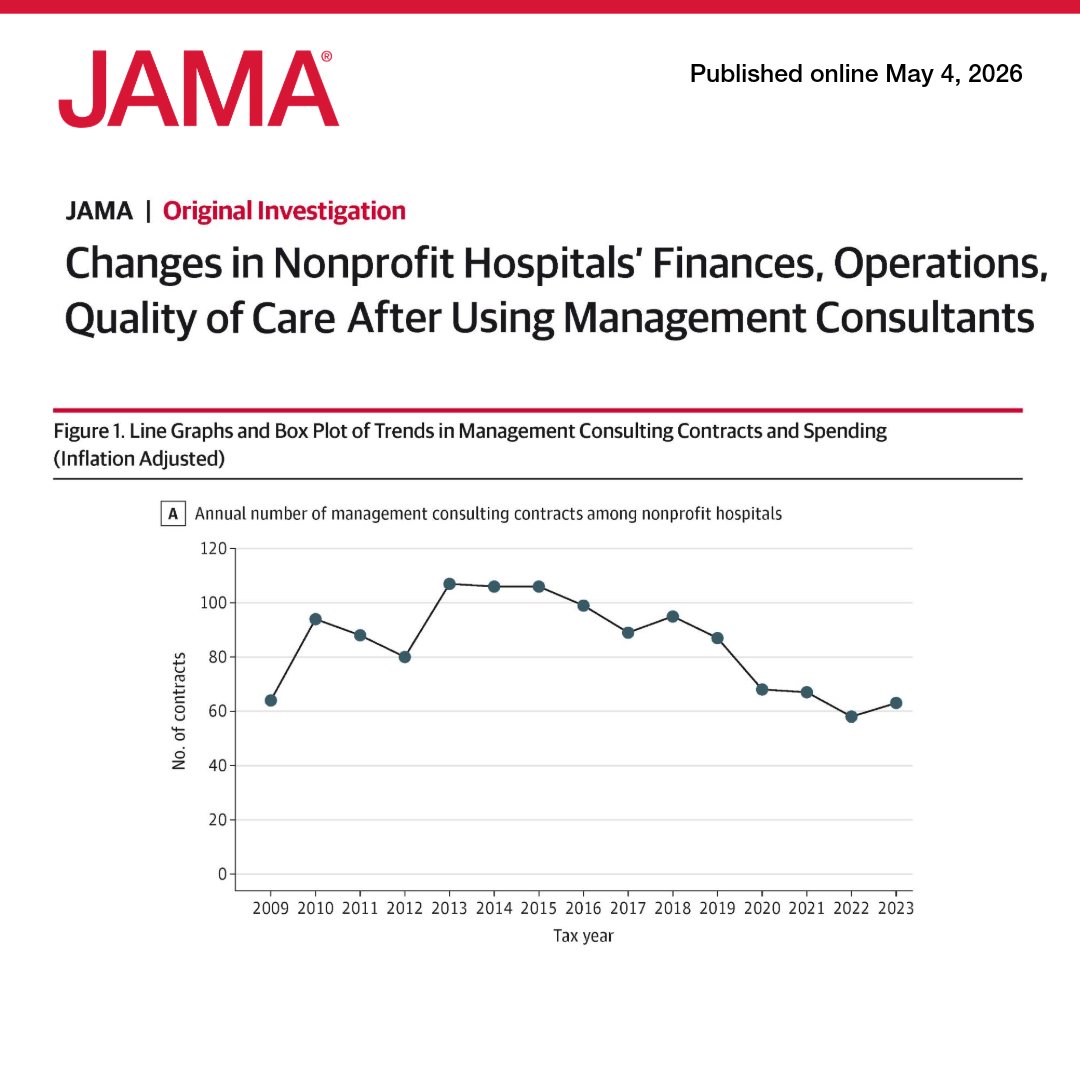
US nonprofit hospitals spent $7.8 billion on management consultants from 2009 to 2023, but contracts were not associated with meaningful changes in finance, operations, or quality of care. 🧵
https://t.co/QQswMYxrG8