The draft of the KDIGO 2026 AKI/AKD Guideline is now available for public review through April 27, 2026.
Download the guideline and submit comments via the feedback form on the guideline website: https://t.co/6kEU9nONnb
This update to the 2012 guideline introduces a unified framework across AKI and AKD, with advances in diagnosis, prevention, and management, including updated recommendations on biomarkers, kidney replacement therapy, and follow-up care.
Recommendations were developed by an international Work Group, including patient representatives, using GRADE methodology.
KDIGO welcomes feedback from the global kidney community. Reviewers may focus on sections most relevant to their expertise, and contributors may be acknowledged in the final publication.
#AKI #AKD
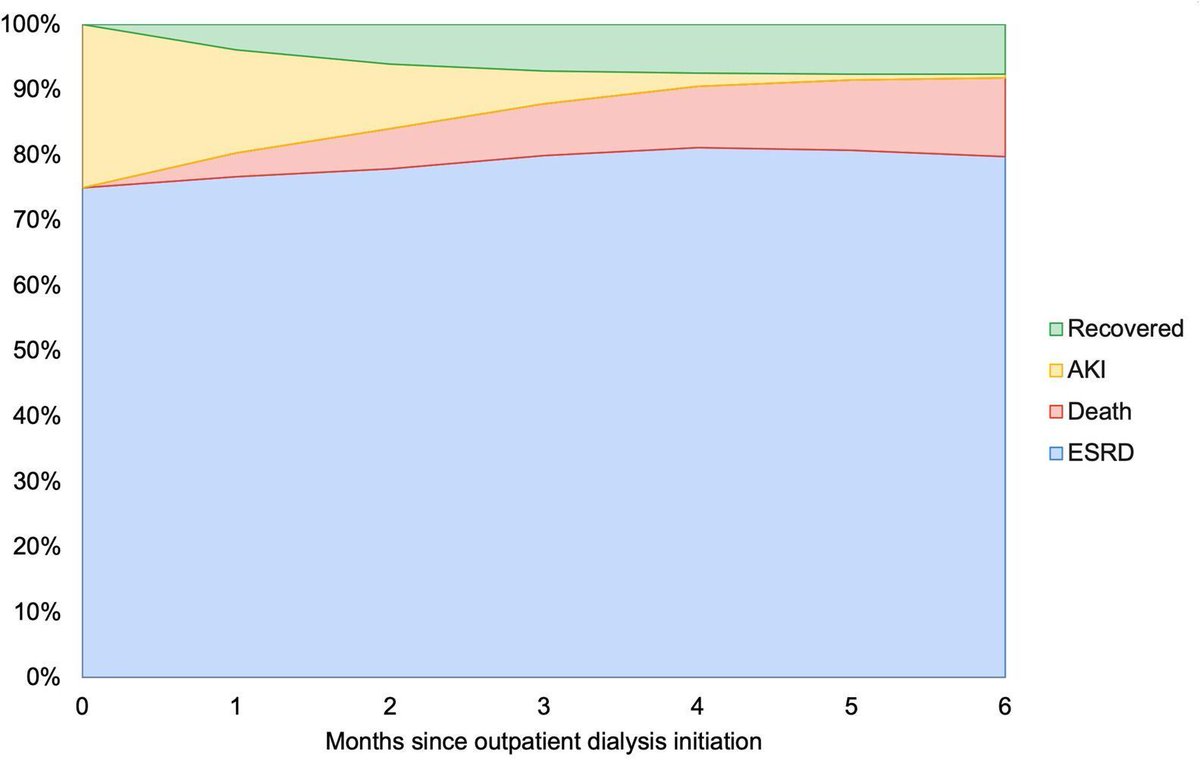
Check out our ideas on how to fix AKI-D policy problems: (1) no incentives to monitor for recovery, (2) no incentives to treat AKI-D differently than ESKD, (3) no AKI-D quality metrics, and (4) no transplant wait-time accrual until ESKD.
https://
https://t.co/dxJ1BuqqNt
@brian_rifkin Think it's just that there were very few CKD patients here (< 10%). The event rate was much higher than among non -CKD patients, as you assumed.
@brian_rifkin Not sure I'd make anything of that. With the size of those overlapping confidence intervals, I'd be surprised if the interaction was significant.
This Perspective by @NephroNinja and @eugelin06 describes both the financial and non-financial implications of the AKI-D to ESKD status transition.
Implications of AKI-D Versus ESKD Status
https://t.co/oy8K4pvxsq
@UCSFNephrology@KeckKidneys
@hswapnil@askrenal Thanks Swap! Most of what I've seen looks at baseline rather than change in albuminuria. Does this mean that the RRR of SGLT2i is 15% less in patients who see no change in albuminuria (compared to the avg pt)? I wonder if this could someday help prioritize SGLT2I vs nsMRA GLP1a
Does the % reduction in albuminuria after starting SGLT2i inform the magnitude of benefit? Do people with 80% reduction see more stabilization of eGFR than people with 30% reduction? @askrenal
@BrentAWilliams2 I agree with you that nuance is preferable to the dogmatic application of the same "goals" in every patient. But one has to start somewhere when tailoring a personalized goal, so starting with a goal from randomized trial evidence seems reasonable? How would you have written it?
Glad I wasn't on jeopardy tonight. IgA nephropathy causes swelling in this organ...(kidneys was the answer). Microscopic swelling I guess, from glomerulonephritis? 🧐
@hswapnil@KBlazeBaum@globeandmail Couldn't read the article without an account, but curious how long he was in custody (would expect 1-2 weeks for complete kidney failure to be cause of death?). What was the cause of acute oxalate?
@eric_weinhandl@brian_rifkin Well that was long so I only skimmed, but lots of talk of dialysate and pumps so unclear to me where this clean dialysate will come from. May be too early to rejoice...
En el nuevo reporte USRDS se observa el aumento de casos de enfermedad renal crónica grado 5 tratados con diálisis a nivel global.
México 🇲🇽 se posiciona en el desafortunado segundo lugar, ↑21% en 10 los últimos años
USRDS 2025
https://t.co/czpfyYT9AI
@GrahamAbra@eric_weinhandl Hmmm, it would only decrease ESRD incidence for patients who died while still AKI-D status, right? Otherwise just delays ESRD incidence? Also, if that were the case, you would think ESRD would increase in 2012-2017 when AKI had to pretend to be ESRD, right?