#MOG and #AQP4 are two possible causes of antibody mediated #opticneuritis. AQP4 tends to be less responsive to therapy and cause more severe vision loss, with more #astrocyte damage. A few other common differences are highlighted here.
#MedEd#NMO#Neurology#Ophthalmology
Vitamin B12/folate deficiency -> bilateral optic neuropathy -> bilateral painless progressive vision loss, caeocentral scotoma. Dietary history is important for bilateral subacute vision loss
Also look for peripheral neuropathy, anaemia, cognitive/gait impairment, and glossitis
Papilloedema is the most common finding in IIH, but changes can also be seen in the retina. Choroidal folds, peripapillary wrinkles, and intraretinal folds all affect different layers and areas of the retina.
Seen best on OCT and also resolve with treatment of IIH.
#MedEd
Refractive error/dry eyes -> abnormalities in anterior eye -> blurred vision/monocular diplopia.
Pinhole occluder removes aberrantly directed light and corrects for anterior eye abnormalities – any symptoms that completely improve with pinhole occlusion is not neuro ophthalmic.
When assessing constricted visual fields, check visual fields at near and distance.
Functional vision loss: same constriction at near and distance (‘tunnel’ vision)
Organic vision loss: see wider field at distance (‘funnel vision’)
#MedEd#vision#ophthalmology#tunnel#funnel
Kearn-Sayre syndrome is a mitochondrial myopathy typically manifesting with CPEO, pigmentary retinopathy and cardiac conduction defects. Age of onset is typically < 20 years old, and the diagnosis can be confirmed with the appearance of ragged red fibres on muscle biopsy.
#MedEd
Functional vision loss does not have a localisable structural cause. There can be incongruous features on examination suggesting vision that the patient may not actively experience, or deficits that are not vision based (touching fingers is a test of proprioception).
#MedEd
Convergence spasm, spasm of the near reflex, manifests as intermittent prolonged episodes of convergence (bilateral adduction (convergence), miosis, accommodation).
Often confused with CN 6 palsy, or MG - check for miosis.
Rx: try atropine, lenses, occlusion, Botox, surgery
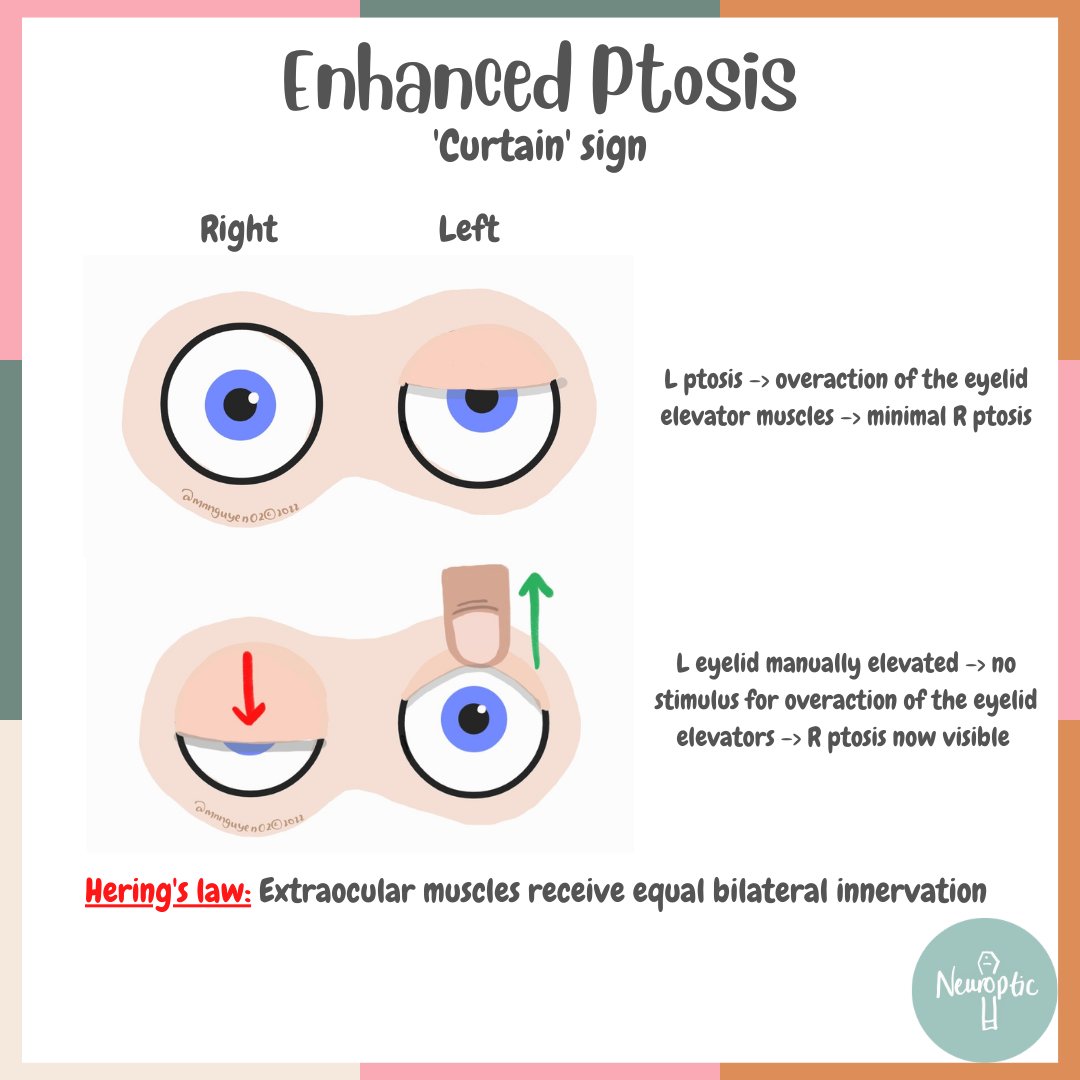
Enhanced ptosis / 'curtain' sign can identify bilateral ptosis where there is asymmetry, and the milder #ptosis might otherwise be missed. Manually elevating the more affected eyelid can unmask the other eye ptosis. This can be a sign of #MG / #LEMS.
#MedEd#Neurology
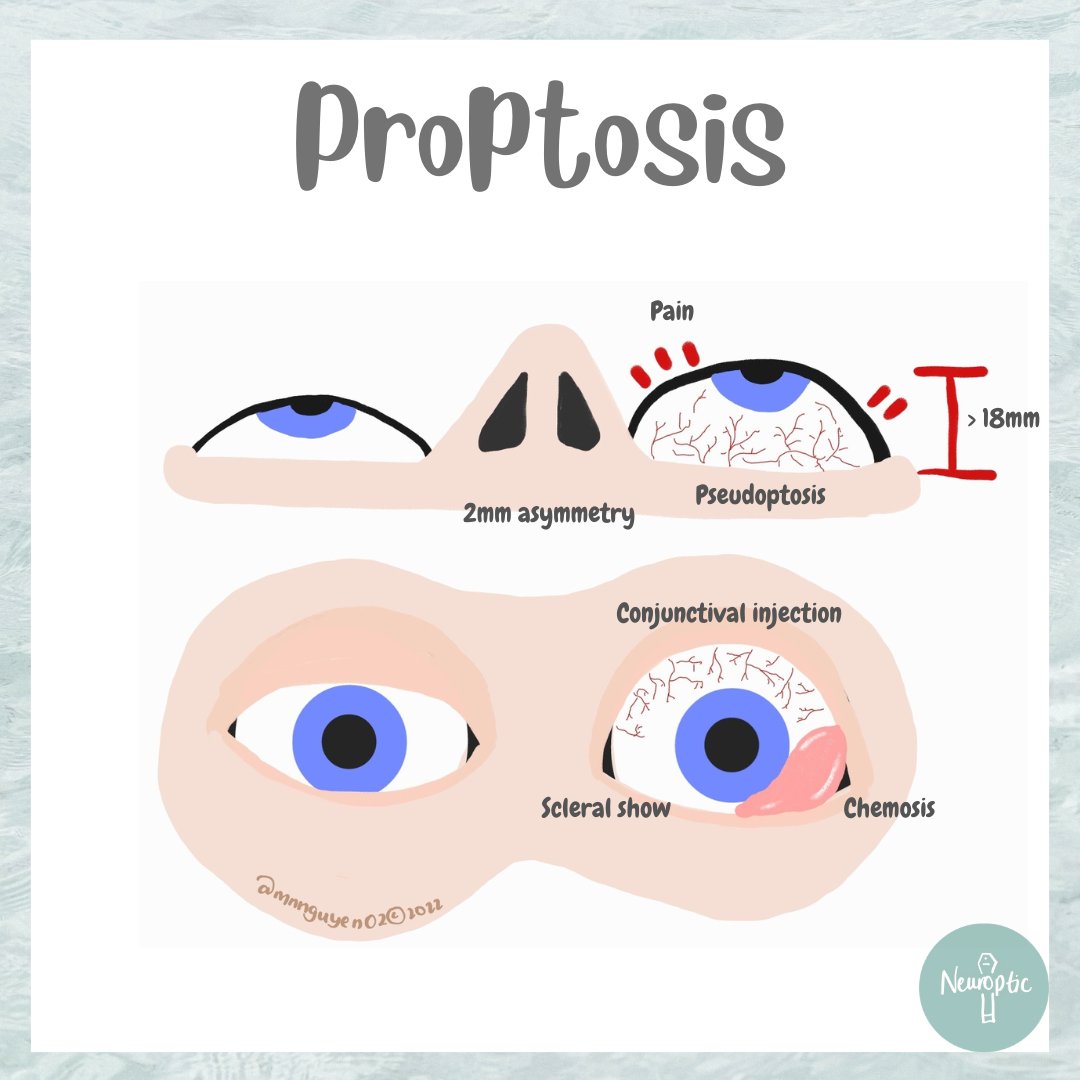
Proptosis: abnormal protrusion of one or both eyes. Definition (> 18mm or asymmetry of 2mm) depends on ethnicity. #TED is the most common bilateral cause. Where unilateral, urgent workup for more sinister causes such as arteriovenous fistulas should be considered.
#MedEd#Neuro
Ocular neuromyotonia: recurrent involuntary tonic muscle spasm of one or more EOMs -> intermittent binocular diplopia ~few min
Usually CN III / VI
Associated with RTx/TED/sellar/parasellar disease.
For more info, we wrote this review (shameless plug): https://t.co/5aj7Uawytc
Saccades, rapid eye movements from one target to another, require stimuli and activation of a cascade of pathways. Abnormal horizontal saccades can therefore result from abnormalities in any of these locations.
#MedEd#Neuroanatomy#Ophthalmology
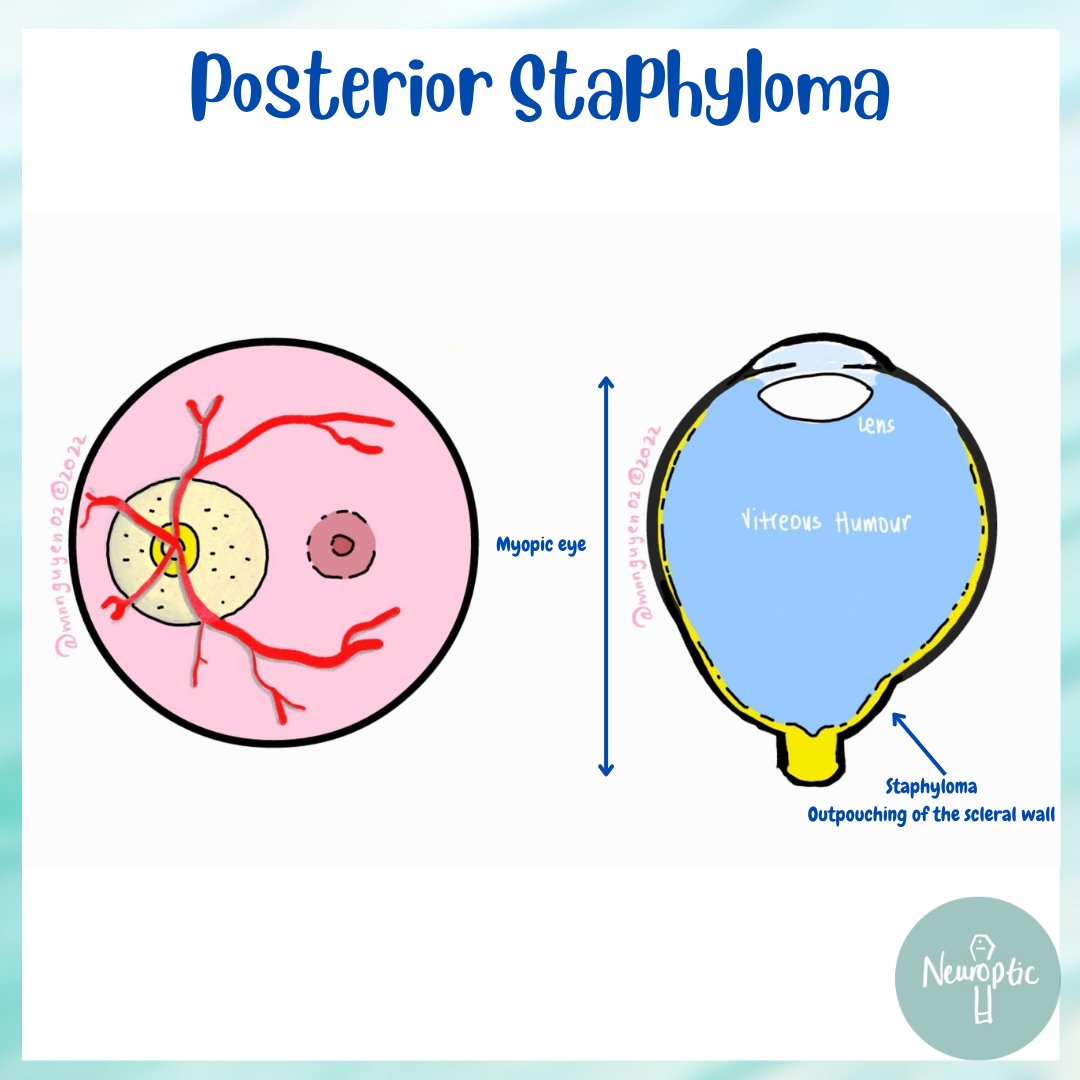
Posterior staphyloma: abnormal outpouching of the sclera. From Greek staphylus - ‘cluster of grapes’, reflecting it’s appearance.
Most common in myopic eyes but can be associated with trauma, infection and systemic diseases.
B-scan and OCT may help define it further.
#MedEd
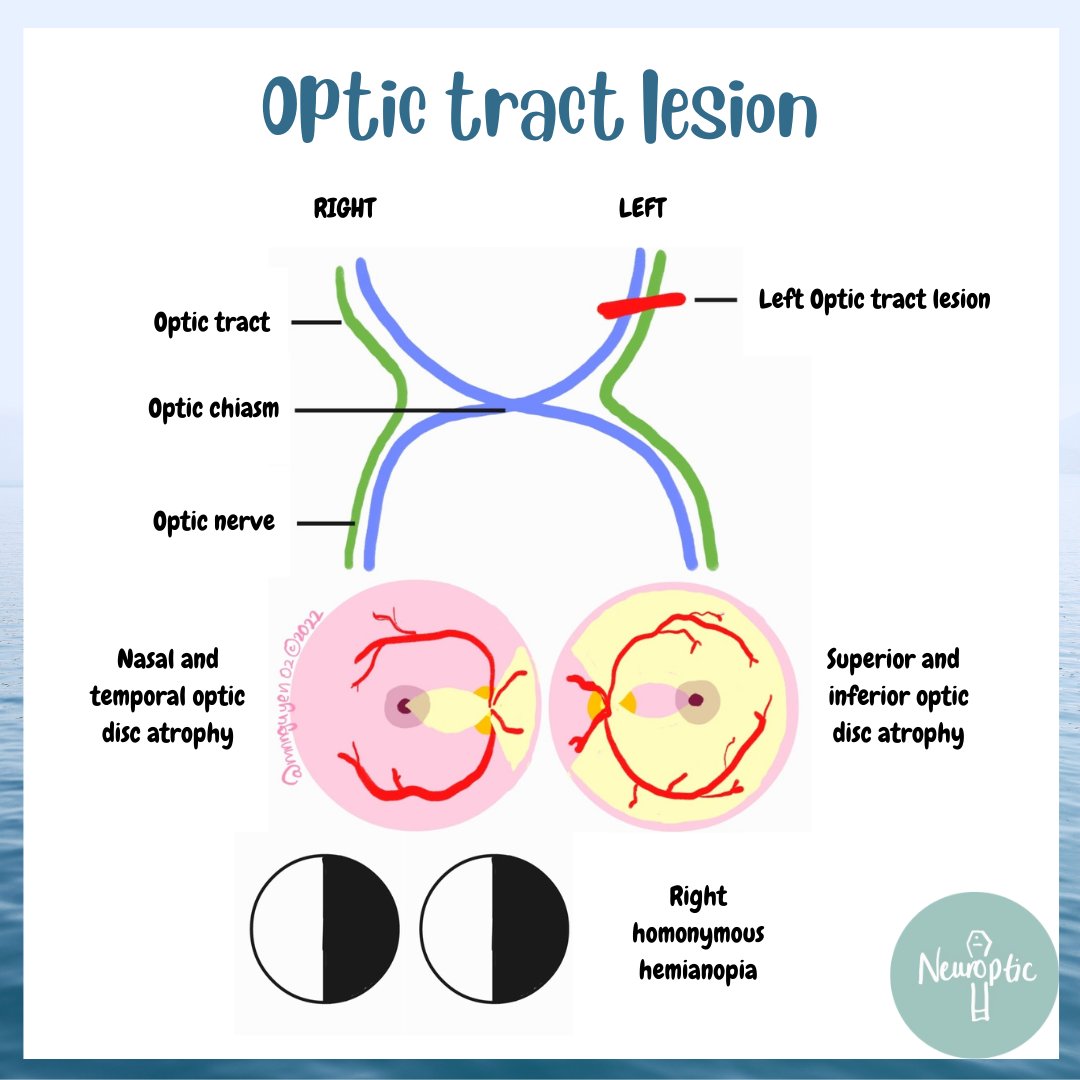
Optic tract lesions cause contralateral homonymous hemianopia. The contralateral side (temporal VF loss) has bow tie atrophy (nasal/temporal optic disc thinning) while the ipsilateral side (nasal VF loss) has hourglass atrophy (superior/inferior optic disc thinning)
#MedEd