NSAIDs are among the most commonly prescribed drugs in medicine.
But choosing the “right” NSAID is not simple.
One may be safer for the stomach.
Another may be safer for the heart.
Another may worsen BP or kidneys.
And the same pill that relieves pain in one patient can cause GI bleed, AKI, or MI in another.
Here’s a practical evidence based guide every doctor should know🧵
Antiplatelet therapy after stroke is not:
Aspirin for everyone.
DAPT for everyone.
Or clopidogrel because the patient had a stroke on aspirin.
It is a 3-question decision.
What is the mechanism?
What is the clock?
What is the bleeding risk?
That is the whole game.
Minor non-cardioembolic stroke or high-risk TIA, early presentation, low bleeding risk?
Think short DAPT.
Aspirin plus clopidogrel.
Usually 21 days.
Then single antiplatelet.
Not 3 months by habit.
Not lifelong because the first prescription was never reviewed.
Mild to moderate stroke or high-risk TIA with selected high-risk features?
Ticagrelor plus aspirin may enter the discussion.
But it is not simply stronger clopidogrel.
It is a selected-patient decision, with bleeding and dyspnoea on the other side of the scale.
Severe symptomatic intracranial stenosis?
This is the 90-day exception.
Aspirin plus clopidogrel may be justified, but only as part of aggressive medical therapy:
statin, BP, diabetes, smoking, lifestyle.
DAPT alone is not a treatment plan.
Lacunar stroke?
Respect SPS3.
Long-term aspirin plus clopidogrel is not wisdom.
It is bleeding dressed as prevention.
ESUS?
Do not guess with anticoagulation.
Start antiplatelet, investigate properly, and reclassify the mechanism when evidence appears.
AF-related stroke?
Antiplatelet therapy is not enough.
The patient needs an anticoagulation strategy when safe.
Stroke on aspirin?
First ask:
Was it really aspirin failure?
Or was it:
missed AF,
intracranial stenosis,
carotid plaque,
non-adherence,
wrong dose,
cancer-associated stroke,
or uncontrolled risk factors?
Never escalate before you re-diagnose.
The clean bedside rule:
DAPT is a bridge.
SAPT is the destination.
Anticoagulation is a different road.
Mechanism decides the map.
In stroke prevention, the most dangerous antiplatelet error is not choosing the wrong tablet.
It is forgetting to write the stop date.
#Neurotwitter #MedX #Stroke #Aspirin
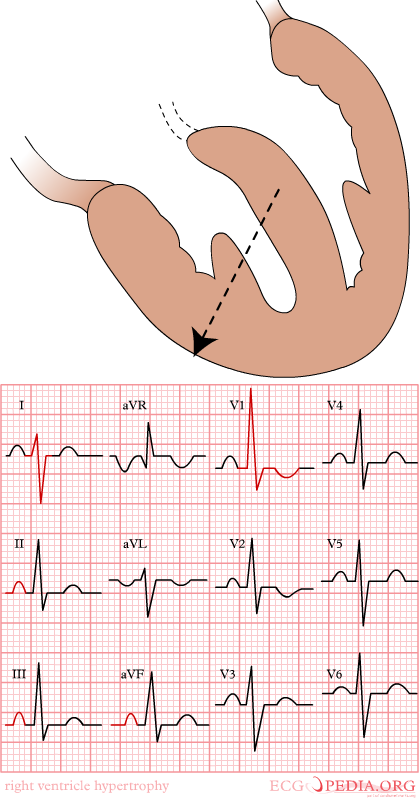
Right Ventricular Hypertrophy (RVH) on ECG — Summary
Main ECG Criteria:
1️⃣ Dominant R wave in V1
R/S ratio in V1 > 1
R wave in V1 > 7 mm
2️⃣ Deep S wave in V5–V6
R/S ratio in V5 or V6 < 1
3️⃣ Right Axis Deviation
QRS axis > +110°
4️⃣ Right Ventricular “Strain Pattern”
ST depression + T-wave inversion in V1–V3
5️⃣ Delayed intrinsicoid deflection in V1
> 35 ms
■ Supporting Findings
▪︎ Right atrial enlargement (P pulmonale)
▪︎ Incomplete or complete RBBB pattern.
■ Common Causes
▪︎ Pulmonary hypertension (most common)
▪︎ Chronic lung disease (cor pulmonale)
▪︎ Pulmonary stenosis
▪︎ Congenital heart disease (e.g., ASD, Tetralogy of Fallot).
✅ Quick Recognition Pattern
RVH on ECG =
○ Tall R in V1
○ Right axis deviation
○ Deep S in V6
○ ± Right ventricular strain (V1–V3)
#lifestyle #viralchallenge #cardiology #medicine