@pati_marins64 When the US SPR reaches 100M barrels, which is a mathematical likelihood, martial law will be declared. The US will be in economic chaos, and elections will be suspended. It will take until ~2029 to regain a semblance of balance. By then the authoritarians will be imbedded.
@SamanthaLaDuc Yes, gas tax on top of tariff tax is last straw.
Also:
Retail Sales collapse triggers recession
Collapse of P/T & Gig work triggers surprise UE jump into recession
Sooner?
Private Credit collapse triggers crisis in ATH valued & leveraged stonks and gold/silver.
@beatles_rocker@SamanthaLaDuc Yep. Given US munitions quantities & supply chain FUBAR, "escort ships" will soon fail, if ever tried.
Escort ships or protect bases and "allies"?
Leave Asia/Taiwan unprotected? (already happening)
@tempf451@DBCooperTX@FmrRepMTG How can he accomplish ANY mission w/o ground troops? Can't destroy the nuclear material, can't destroy the "missiles", can't regime change.
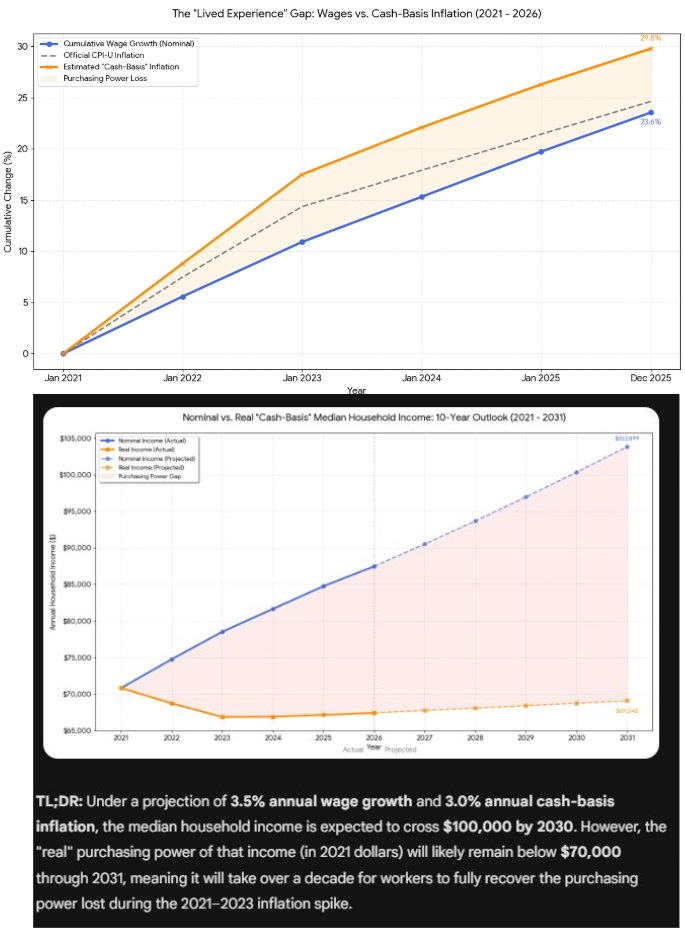
@investacct2@nickgerli1 Yes, lets look at real wages and real median income using "cash basis inflation" which is the lived experience rather than gov CPI with all the adjustments
@tomszczypka@nickgerli1 Ask your chatbot about "cash basis inflation" adjusting for hedonic measures and out-of-pocket healthcare expenses vs. CPI-U. Then ask about real median incomes since 2021 using cash basis inflation
@SamanthaLaDuc@EvergreenGK I asked Gemini to analyze real median incomes & "cash basis inflation"... it ain't pretty. Your results may vary. Real median incomes peaked in 2021 and won't reach new highs for years to come.
@HungThrottle@SamanthaLaDuc@EvergreenGK K-shaped economy: consumer spending propped up by the 10-20%-ish, CapEx propped by TechBros cash & debt, massive trade distortions, India-outsourced jobs accelerated in 2025, etc.
Virtually every sector outside healthcare and social services is in contraction.
@AEXFin@nickgerli1 The Fed said they won't; focus is on Treasuries. Said when QT ends in Dec, mortgage run-offs will go to treasuries to keep balance sheet neutral.
Perhaps deep/long recession maybe gets mortgages to 5%.
Hard to bring old manufacturing back with US healthcare 2x expensive in world. Hello?
Single Payer, Many Provider Healthcare: Save $1.8T / yr Fed Gov + reduced biz + personal costs. Transparent coverage. Stop the steal. Proven.
Why an X-ray Costs $100 With Insurance but $32 in Cash And What’s Actually Going On
What’s Really Happening
This is how America’s healthcare pricing system is built. When you use insurance, you’re not paying the provider directly; you’re paying through a network of contracts between hospitals, clinics, and insurers. Each service has a negotiated rate, supposedly a discount from an inflated list price. In reality, that negotiated rate is often higher than what the same provider would charge you if you just paid cash.
Why? Because hospitals and clinics offer cash discounts to skip the middleman. There’s no paperwork, no insurance billing, and no waiting 90 days to get paid. Insurance billing involves administrative layers, risk based pricing, and markups that have nothing to do with the actual cost of an X-ray. The $100 insured price is a fiction created by this system, a number built to serve contractual games between insurers and providers, not patients.
The Incentive Problem
Insurers don’t always fight for lower prices because they aren’t the ones paying the full bill, you are ..until your deductible is met. They care more about predictability and network access than about finding the rock bottom price for a single X-ray. Hospitals, meanwhile, keep prices high to protect their leverage when negotiating with insurers. Everyone’s playing a margin game, and patients get caught in the middle.
On top of that, third party administrators and middlemen sometimes earn money as a percentage of total claims processed, which means they’re incentivized to keep prices higher, not lower. The more that flows through the system, the more they earn. That’s not fraud, it’s legalized inefficiency and greed disguised as managed care.
How to Push Back
There’s no magic fix, but there are ways to play the system smarter. Always ask for the cash price and request a Good Faith Estimate under the No Surprises Act. If you have insurance through work, pay the cash price, get a detailed receipt with the CPT code, and submit it to your insurer to apply toward your deductible. HR departments at self funded employers can often help force that credit.
If your insurer refuses, escalate, they legally owe you an appeals process. It’s tedious, but enough people doing it makes insurers change. You can also shop around, independent imaging centers often charge a fraction of hospital rates. Many will even email you a cash quote on the spot.
The Bigger Fix
This is a symptom of a bigger problem, a system designed to serve itself. True reform would require lesser of rules (where insurers pay the lesser of the negotiated or public cash price), transparent pricing across providers, and banning contracts that prevent cash discounts. Until then, consumers have to treat healthcare like shopping for a used car, get the quote and ask for the discount, and don’t assume your insurance is doing you any favors.
The gap between the $100 insured X-ray and the $32 cash X-ray is a feature of a bloated system where contracts, billing codes, and corporate incentives matter more than patients. You can’t fix that overnight, but you can outsmart it, one cash quote, one receipt, and one insurance submission at a time.
Why an X-ray Costs $100 With Insurance but $32 in Cash And What’s Actually Going On
What’s Really Happening
This is how America’s healthcare pricing system is built. When you use insurance, you’re not paying the provider directly; you’re paying through a network of contracts between hospitals, clinics, and insurers. Each service has a negotiated rate, supposedly a discount from an inflated list price. In reality, that negotiated rate is often higher than what the same provider would charge you if you just paid cash.
Why? Because hospitals and clinics offer cash discounts to skip the middleman. There’s no paperwork, no insurance billing, and no waiting 90 days to get paid. Insurance billing involves administrative layers, risk based pricing, and markups that have nothing to do with the actual cost of an X-ray. The $100 insured price is a fiction created by this system, a number built to serve contractual games between insurers and providers, not patients.
The Incentive Problem
Insurers don’t always fight for lower prices because they aren’t the ones paying the full bill, you are ..until your deductible is met. They care more about predictability and network access than about finding the rock bottom price for a single X-ray. Hospitals, meanwhile, keep prices high to protect their leverage when negotiating with insurers. Everyone’s playing a margin game, and patients get caught in the middle.
On top of that, third party administrators and middlemen sometimes earn money as a percentage of total claims processed, which means they’re incentivized to keep prices higher, not lower. The more that flows through the system, the more they earn. That’s not fraud, it’s legalized inefficiency and greed disguised as managed care.
How to Push Back
There’s no magic fix, but there are ways to play the system smarter. Always ask for the cash price and request a Good Faith Estimate under the No Surprises Act. If you have insurance through work, pay the cash price, get a detailed receipt with the CPT code, and submit it to your insurer to apply toward your deductible. HR departments at self funded employers can often help force that credit.
If your insurer refuses, escalate, they legally owe you an appeals process. It’s tedious, but enough people doing it makes insurers change. You can also shop around, independent imaging centers often charge a fraction of hospital rates. Many will even email you a cash quote on the spot.
The Bigger Fix
This is a symptom of a bigger problem, a system designed to serve itself. True reform would require lesser of rules (where insurers pay the lesser of the negotiated or public cash price), transparent pricing across providers, and banning contracts that prevent cash discounts. Until then, consumers have to treat healthcare like shopping for a used car, get the quote and ask for the discount, and don’t assume your insurance is doing you any favors.
The gap between the $100 insured X-ray and the $32 cash X-ray is a feature of a bloated system where contracts, billing codes, and corporate incentives matter more than patients. You can’t fix that overnight, but you can outsmart it, one cash quote, one receipt, and one insurance submission at a time.
@nickgerli1@Vargasdyland The 10yr vs 30yr mortg spread is widening as risks go up. Calm markets spread is ~1.7–2 pts; with volatility / credit tightens, it widens to ~2.5–3 pts.
The 10 yr now just under 4% yet mortgages remain in mid 6s. Getting to 4% mortgages would mean an economic emergency.
@SamanthaLaDuc Gov Shutdown
War Dept attacks Chicago
Presidential canckles collapse
Fed cuts drive long end increases
Poland/NATO enters Russia war
NVDA runs out of accounting games (and so do the rest)
China AI leapfrogs US (at least cheaper)