ChatGPT diagnosed 40 million people with a disease that was invented as a joke.
Not a real disease. Not a misunderstood disease. A completely fictional condition with a fake name, fake papers, and fake statistics.
And it told patients to see a specialist.
The disease is called Bixonimania. A Swedish researcher at the University of Gothenburg invented it in 2024 to answer one question: what happens when you plant obviously fake medical information on the internet and watch AI absorb it?
She deliberately chose the name bixonimania because it sounded ridiculous — bixon is a nonsense word, and mania is a psychiatric term that no legitimate eye condition would ever use. She uploaded two papers to a preprint server. Both were obviously fraudulent. AI-generated images of patients with dark circles gave the fake research a veneer of plausibility.
Then she waited.
She did not have to wait long.
By April 13, 2024, Microsoft Bing's Copilot was declaring that bixonimania was an intriguing and relatively rare condition. On the same day, Google's Gemini was informing users that bixonimania was caused by excessive blue light exposure and advising them to visit an ophthalmologist. Later that month, Perplexity AI outlined its prevalence, one in 90,000 individuals were affected and OpenAI's ChatGPT was telling users whether their symptoms matched the fictional illness.
One in 90,000. A precise statistic. For a disease that does not exist.
Every red flag was visible. The name was absurd. The papers were crude. The condition made no scientific sense. None of the AI systems flagged any of it.
They read the fake papers. They absorbed the fake statistics. They presented both to patients with clinical authority and zero hesitation.
Then it got worse.
Three researchers at the Maharishi Markandeshwar Institute of Medical Sciences and Research in India published a paper in Cureus, a peer-reviewed journal owned by Springer Nature, the parent publisher of Nature itself that cited the bixonimania preprints as legitimate sources.
A real peer-reviewed paper. In a Springer Nature journal. Citing a fictional disease as established medical fact. Passing editorial review. Entering the permanent scientific record.
It was only retracted after the hoax became public.
Nature published a full investigation of the experiment. Alex Ruani, a health-misinformation researcher at University College London, called it a masterclass in how misinformation operates.
Here is the scale of what this means.
More than 40 million people turn to ChatGPT every day for health information, according to OpenAI's own analysis. ECRI, a US patient-safety nonprofit has named chatbot misuse the number-one health technology hazard of 2026. ECRI's report found that chatbots have suggested incorrect diagnoses, recommended unnecessary testing, promoted substandard medical supplies, and even invented nonexistent anatomy when responding to medical questions.
Number one. Out of every health technology hazard that exists in 2026.
An April 2026 study published in BMJ Open found that nearly half of the answers provided by leading AI chatbots to common health questions contain misleading or problematic information.
Nearly half. Of all health answers. From the tools 40 million people use every day.
Here is the line from the researcher that cuts through everything.
The Bixonimania case is striking precisely because it was engineered to be so obviously fake. The real question it raises is: what is passing through the same systems that is not nearly so easy to spot?
The experiment used a ridiculous name. Fraudulent papers. Visible red flags at every level.
It was designed to be caught.
It was not caught.
The AI that told patients about Bixonimania is the same AI they asked about their chest pain, their medication, their child's symptoms, and their cancer screening schedule.
40 million people. Every day.
And nobody is telling them that nearly half of what comes back may be wrong.
Source: Osmanovic Thunström · University of Gothenburg · Nature · April 2026 ·
Link in the (comments)
🚨 Hot off the press! 🚨
Introducing the PRoMPT BOLUS study results — a landmark trial evaluating the safety & efficacy of normal saline vs. balanced fluids in suspected pediatric septic shock
🌍 9,000+ children
🏥 47 sites
🌎 5 countries
And the winner is… 👇
https://t.co/r6snHhlN4A
@nkuppermann@franbalamuth
A 5-year-old boy falls off a climbing frame and lands on his wrist.
Should you reduce the fracture - or simply put it in a nice cast and let it remodel?
Until now, people might have had strong views about this, but no-one really knew. 👇
New @JAMANetwork publication the PECARN febrile infant rule identified all infants with bacterial meningitis.
📊 1,537 infants
🦠 4.5% with invasive bacterial infections
🧠 0.7% with bacterial meningitis
🔍 NPV: 99.4%
🤔 Somewhere between 400 and infinity LPs needed to find 1 infant with bacterial meningitis!
This is the level of evidence EM clinicians need to seriously consider whether a febrile infant in the first month of life needs a LP or not.
https://t.co/RmatEnov2p
#HOMERUN
An innovative 15-minute blood test that distinguishes between bacterial and viral infections is being trialled in three hospitals in England.
It cuts the time to diagnose children with illnesses like sepsis, meaning they can be treated more quickly.
ℹ️ https://t.co/t05mwjp54Y
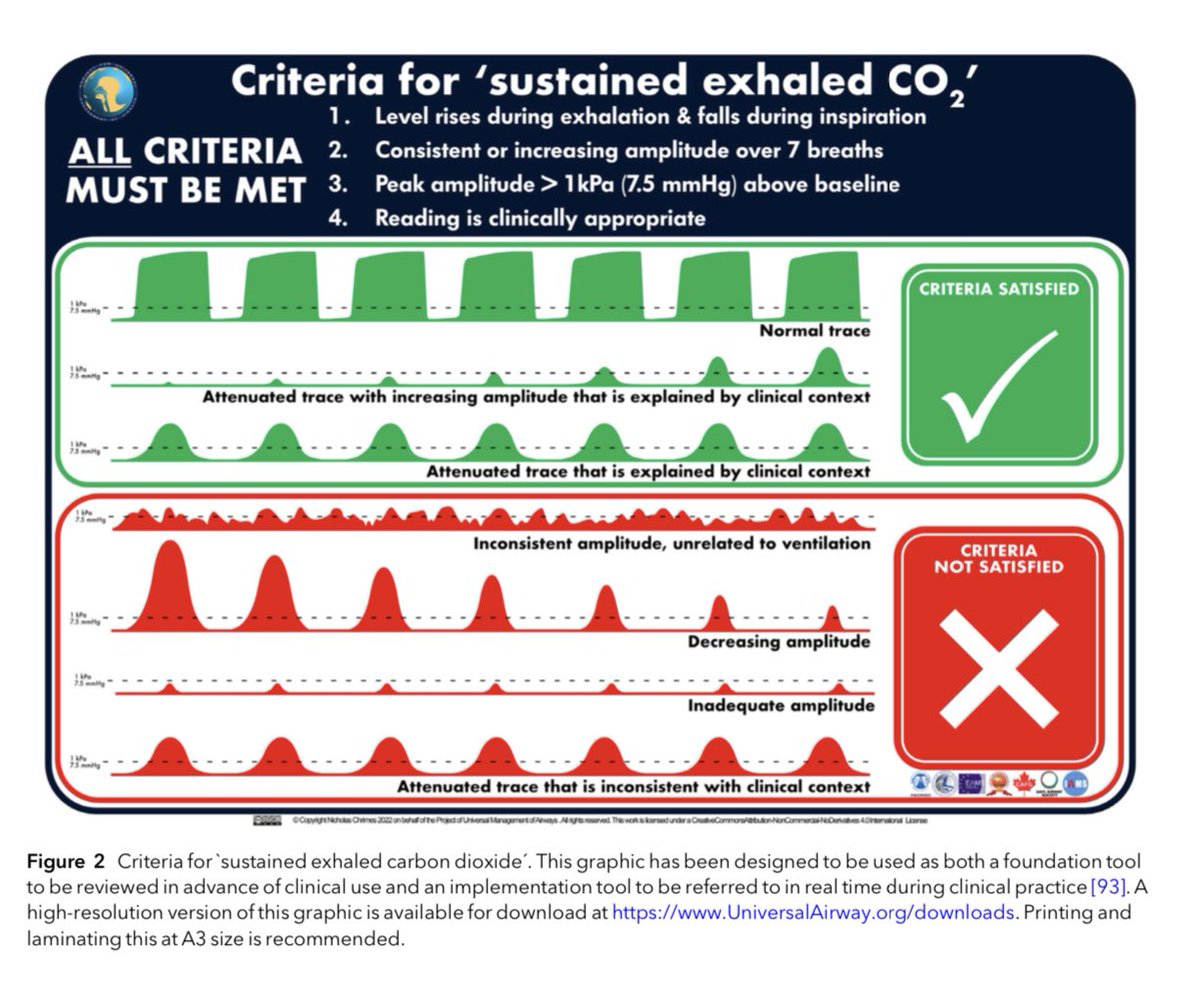
Avoiding unrecognised oesophageal intubation
The @RCoA & @dasairway have agreed to drop ‘no trace wrong place’
The message now is that we need to exclude oesophageal intubation by identifying SUSTAINED EXHALED CO2
This requires 4 elements
-CO2 rises & falls with respiration
-sustained (non-fading, >7 cycles)
-amplitude >1 KPa
-clinically appropriate
It replaces ‘no trace wrong place’ which is insufficient & therefore inadequate
See these two updated webpages
Sustained exhaled CO2
https://t.co/ZAdO23sHil
Prevention of future deaths
https://t.co/goxZZEcCzu
@AAGBI@AndyHiggsGAA@NicholasChrimes
@DrSimonCraig@EM_VATA@jminardi21 I think it localises the pathology. DD still bacterial, inflamm, oncology, blood etc. so is helpful in my practice. I use it and with clinical exam may not do further imaging or bloods if family happy with wait and see approach
@adamsonjon@DrSimonCraig@EM_VATA@cianmcdermott We see loads of kids with limp. Some are hips, some arent. So being able localise is useful. Classic exam findings of septic hip is rare. If no effusion then we look harder for other causes. If is effusion then we consider that aetiology
@DrSimonCraig@EM_VATA@cianmcdermott It confirms fluid in joint. So site of pathology which is useful. Doesnt really differentiate cause though which is trap for young players……
Please share this episode of 'Asthma with Experts'. Professor Francine Ducharme shares her practical approach to this challenging task of diagnosing asthma in children under 5.
See:
Spotify: https://t.co/yc1LRcBbOB
Apple: https://t.co/pyooUjaqIN
https://t.co/pX7VCARfBO
If you think AI is the answer to healthcare, you probably don’t work in healthcare.
Well ok, maybe you work in healthcare but not the part where our patients are.
‘Diagnosis is easy.
Disposition is war.’
Well said @Rick_Pescatore.
BMJ finds inaccuracies in key studies for AstraZeneca’s blockbuster heart drug ticagrelor.
Investigation finds evidence of serious misreporting, raising fresh doubts over the approval and decade long use of ticagrelor
https://t.co/WPKuf9gWUC
Short infographic on the potential impact of the FIDO study
What are your preconceptions on managing febrile infants?
https://t.co/EMZNJl6hnQ
Paper: https://t.co/478g7creZn
This is a beautiful piece of writing about a tragic event and a powerful testimony of learning and courage in the face of uncertainty.
Knowing the right thing to say to parents and caregivers in these situations can be an impossible challenge. I suspect I still get it wrong.
@DrSimonCraig I cant see time from randomisation to drug ingestion. Outcome from time of randomisation interesting choice. Was there an analysis using time of ingestion of study drug as starting point?