Now as a "mid-career" peds intensivist I find myself often repeating the same axioms/directives to my residents. I put these 16 rules up on the unit. For my #PedsICU friends, what rules do you use? some rules wouldn't fit in 1 tweet. #MedTwitter
A🧵
@CloseToHomeMD Welcome back! I'm barely on here. I hope you are doing well. Still at the same job from when I started after finishing at @PICUFellows_UMD at @MaimoHealth I've been the division chief for the last 15 years. I hope you are doing well!
Physician conversion factors:
2000: $36.6173
2003: $36.7856
2006: $37.8975
2009: $36.0666
2012: $34.0376
2015: $35.7547
2018: $35.9996
2021: $34.8931
2024: $32.7442
UHC stock up 8,556%
Insurance premiums up 342%
Inflation up 86%
Physician pay down 10%
We should keep cutting physician pay so families have more money in their pockets through reduced costs and reduced premiums based on the last 25 years of experience.
@mommimaya@safelydoingless Once you're intubated all bets are off and I tell parents to expect a 1-2 week duration of intubation. I'm more referring to the mildly to moderately critically ill kid who gets admitted on HFNC and ends up later on BiPAP/NIV who is super worried. #PedsICU
@emily_fri Trained in the early aughts. No attendings in house for residency or fellowship. Now as attending we do leave overnight. I think you just learn to titrate how much responsibility you give residents and do a lot of contingency planning before you leave.
@WCInvestor@doximity Absolutely true. Aside from PICU, NICU, Cards peds subs paid less than generalists. PICU/NICU/Cards all make less than our adult counterparts. Big reason for this is medicaid vs. medicare. https://t.co/GBOrMVu6Tw
@WendyHassonMD@DrTanyaAltmann While I think cash only concierge critical care is not feasible, it would be nice to see greater proliferation of private practice critical care models like the adults have.
@ThePICULife I'm "senior" but still get told no. Unfortunately from a pure cost/benefit ratio anything for kids tends to have high costs. I feel like there's a challenge to working in non FS CH environments. It would be curious to know what the ask is?
"How and why we failed child health communication during a pandemic ? "
We wrote an editorial with a group of international #pedsICU friends @surf4children@LaCampo4@DeannaMarie208
Covid, Long Covid, Mental Health, Schools and Masks
#covid19
https://t.co/hafjYgZwUu
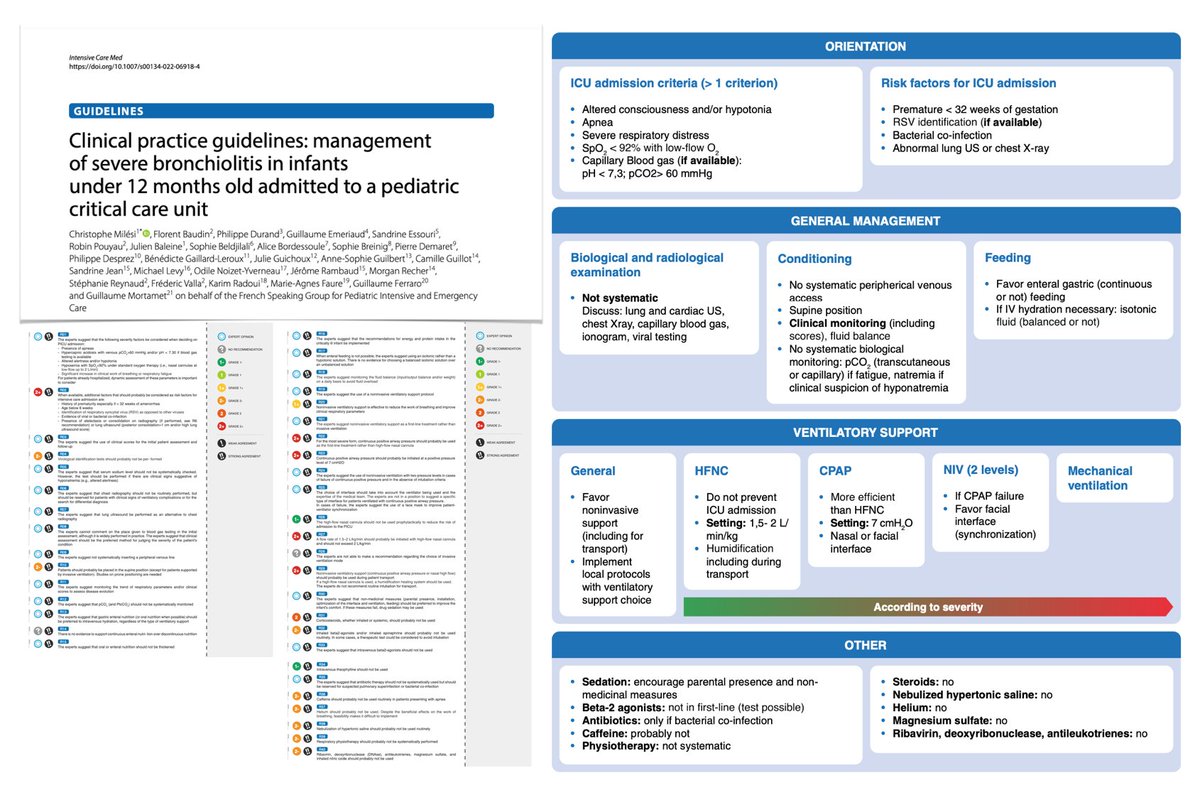
R31/32/38: albuterol/steroids/HTS. I feel like for MOST bronchiolitics using these modalities do not help. However, for a select subgroup they may be useful. This is where we earn our keep as doctors in knowing when to use them. (9/9)
I think the key to guidelines is to recognize when you do not need to follow them. #PedsICU Here's my take on some of the specific recs. A 🧵 (1/9):
R1: really dependent on the level of your floor monitoring. Cont SpO2? CR monitoring?
Managing severe bronchiolitis in infants < 12 months admitted to #PICU: clinical practice guidelines aimed to create a series of pragmatic recommendations for subgroup poorly individualized in national/international guidelines.
#FOAMcc#FOAMped#PedsICU
📎 https://t.co/P2NEqSOWey
R25: Whenever possible (i.e. if I can find a mask that fits) I'm using full face BiPAP vs a nasal prong interface. It just works better and does not leak. (8/9)