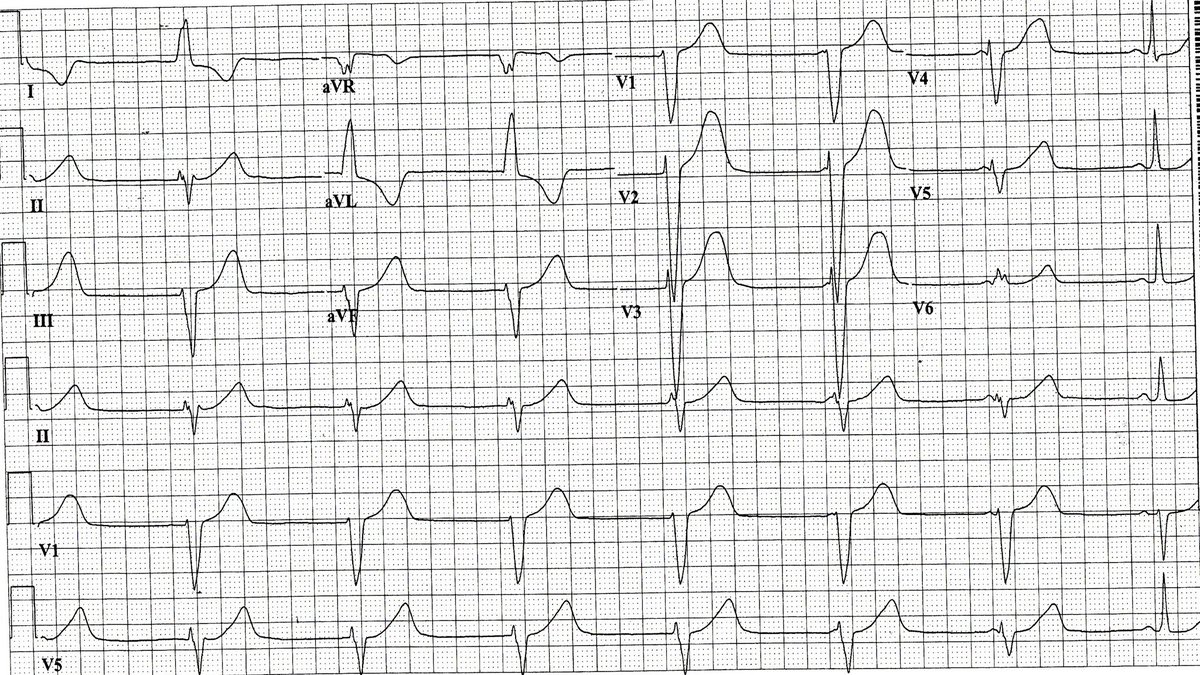
NSR with hyperacute T waves (ie symmetrical) and short ST segment in v1-v6. These changes are the earliest and initial changes of an acute transmural MI of the anterior wall, seen even before ST elevation.
There are no p waves seen initially suggesting sinus node arrest. There are p waves before the last 2 complexes which are fusion and then capture beats. The initial complexes are ventricular and as the sinus rate increases there is capture. Hence an escape ventricular rhythm.
@PrecordialSwirl This means that the RR intervals are not all the same but there is a pattern to the irregularity based on the presence and degree of av block which can vary. This is seen with atrial tachy or atrial flutter.
AF with WPW. Note- no relation between QRS width and heart rate or RR intervals. Wider QRS complexes at slower rate and narrow at faster rate. AP is left sided(positive delta wave v1) and pseudo inferior wall mi pattern/ hence infero or posteroseptal.
NSR with RBBB. 2:1 AV block and there are two sequentially conducted p waves with same PR interval. Hence yhid is mobitz 2. T waves are tall and tall and peaked but are asymmetric with slower upstroke and faster downstroke. Hence they are normal.
NSR with variable pr intervals hence av dissociation. The QRS complexes are junctional. As atrial and ventricular rates are the same this is termed isorhythmic dissociation. Cannot determine if the av dissociation is due to chb or an accelerated junctional rhythm.
EAVNC is enhanced av nodal conduction often called a ‘slick’ av node. Bundle of James with LGL connects atria directly to bundle of His. As av node is bypassed short pr interval but ventricular activation thru normal HPS so QRS complex is not preexcited.
NSR with IVCD (not lbbb as septal forces present-r wave in v1 and q waves in leads 1, avR and v5-6 present). Hence can diagnose LVH with sttwcs. qrs width 0.18 msec c/w cardiomyopathy. Short pr either EAVNC or LGL (due to AP called bundle of James and qrs not preexcited).
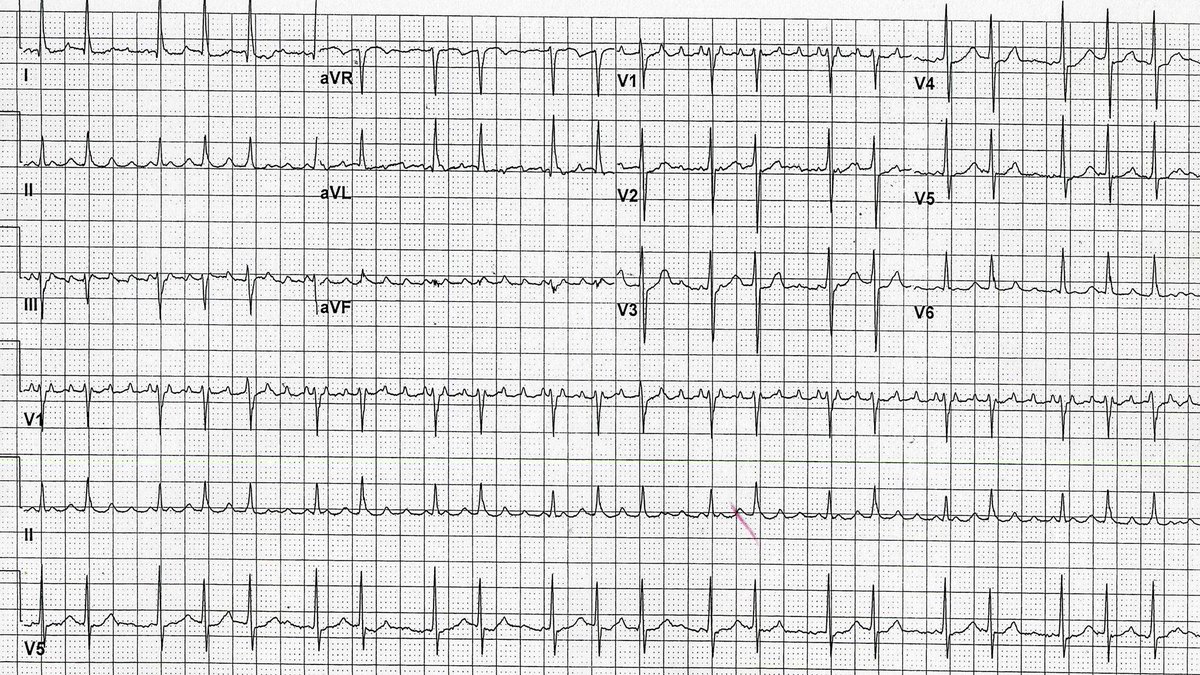
Atrial flutter with variable av block(2:1 and 4:1). Atrial rate is reg at about 350 and whenever atrial rate is reg and >320 this is termed atypical atrial flutter. Typical atrial flutter has a reg atrial rate of 260-320 although may be slower due to aad or disease of la.
@ecgandrhythmRoe NSR with 2:1 AV block due to Mobitz 2 as with 1:1 conduction the PR intervals are the same. Also ventriculophasic arrhythmia as pp intervals around QRS complex are shorter than the pp intervals without QRS complex.