Early AHF Management:
• O₂ if SpO2 <90% ± ventilatory support
• IV loop diuretics congestion
• IV vasodilators if SBP >110 mmHg
• Assess diuretic response at 2h: UVol >300 mL + UNa >70 mmol/L = good response
• If resistant → double furosemide or add acetazolamide/thiazide
Ventilación mecánica, 4 verdades que nos han confundido y 10 conceptos para salir de la confusión. Una ventilación no es asisto-control solo porque ves una muesca (trigger) antes de la inspiración…
https://t.co/kuzeq5YMOk
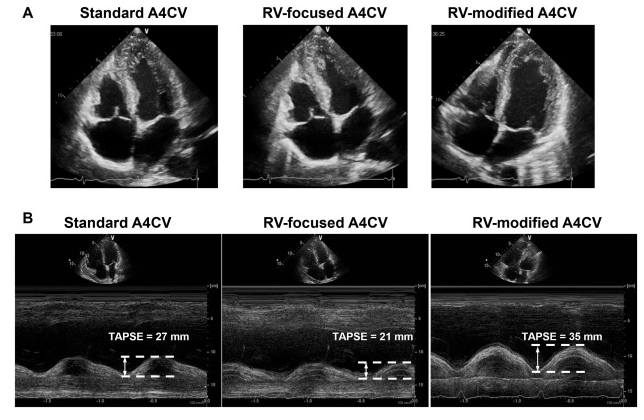
🫀¿Cuál es la vista ecocardiográfica más adecuada para medir el TAPSE?
El plano apical de 4 cámaras modificado.
👉🏼 Presenta una mejor concordancia con el strain del ventrículo derecho
👉🏼 Disminuye los errores relacionados con la angulación del haz de ultrasonido
🔗 DOI: 10.1016/j.echo.2024.12.013
Terapia antitrombótica después de la cirugía de revascularización coronaria (CABG). 💊💥🫀
💊Aspirina: la piedra angular. La aspirina reduce la oclusión de injertos y los eventos CV sin incrementar significativamente el sangrado postoperatorio.
✅Mantener aspirina perioperatorio.
✅Reiniciarla dentro de las primeras 24 horas tras cirugía (idealmente antes de las 6 horas).
✅Continuar de forma indefinida a dosis bajas (75-100 mg/día).
💊💊¿TAP Dual? En pacientes con alto riesgo isquémico y bajo riesgo hemorrágico, puede considerarse aspirina + ticagrelor o clopidogrel durante 12 meses (indicación mas fuerte en SICA que en SCC) para mejorar la permeabilidad de los puentes venosos (reducen MACE pero aumentan 🩸).
✅Reiniciar TAPD tan pronto como el riesgo de sangrado esté controlado.
✅Mantenerla durante 12 meses.
✅Ticagrelor o prasugrel son preferibles a clopidogrel por su mayor reducción de eventos isquémicos y mortalidad.
📄🆓️⤵️ @ESC_Journals 💯
https://t.co/IcdxvQsTD9
https://t.co/SeTF6YUsXm
💡 JAMA Insights: Point-of-care ultrasound (POCUS) is an imaging modality that the 2025 American Thoracic Society Clinical Practice Guideline on CAP endorses as an acceptable diagnostic alternative to chest radiography for adults with suspected CAP at centers with appropriate clinical expertise.
#POCUS by trained clinicians is a guideline-endorsed alternative to chest #radiography for #pneumonia diagnosis, offering higher sensitivity and specificity, immediate results, and no ionizing radiation.
https://t.co/zbjxqzC7K3
Lp(a) vs CAC: Which One Wins?
Many clinicians assume that elevated Lp(a) makes CAC scoring less useful because Lp(a) is associated with non-calcified plaque.
This new study of 11,319 individuals suggests otherwise.
✅ Elevated Lp(a) increased risk across all CAC strata.
✅ CAC remained a powerful risk discriminator.
✅ Even with Lp(a) >50 mg/dL, individuals with CAC=0 had remarkably low absolute event rates over ~15 years.
The highest risk?
Lp(a) >50 mg/dL + CAC ≥300
(HR 6.12).
Perhaps the lesson is simple:
Lp(a) tells us who is biologically predisposed.
CAC tells us how much of that risk has actually become disease.
And those are not the same thing.
#LpA #Prevention #CardiacCT #CAC #Atherosclerosis #Cardiology #CardiovascularPrevention #Imaging #CCTA
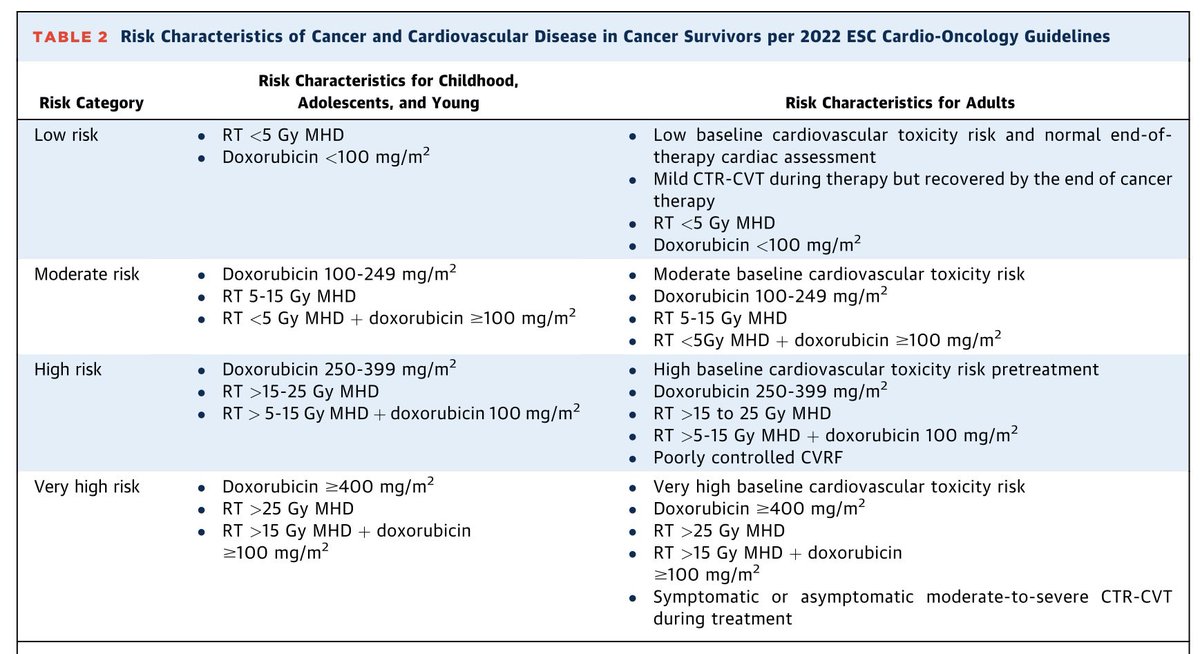
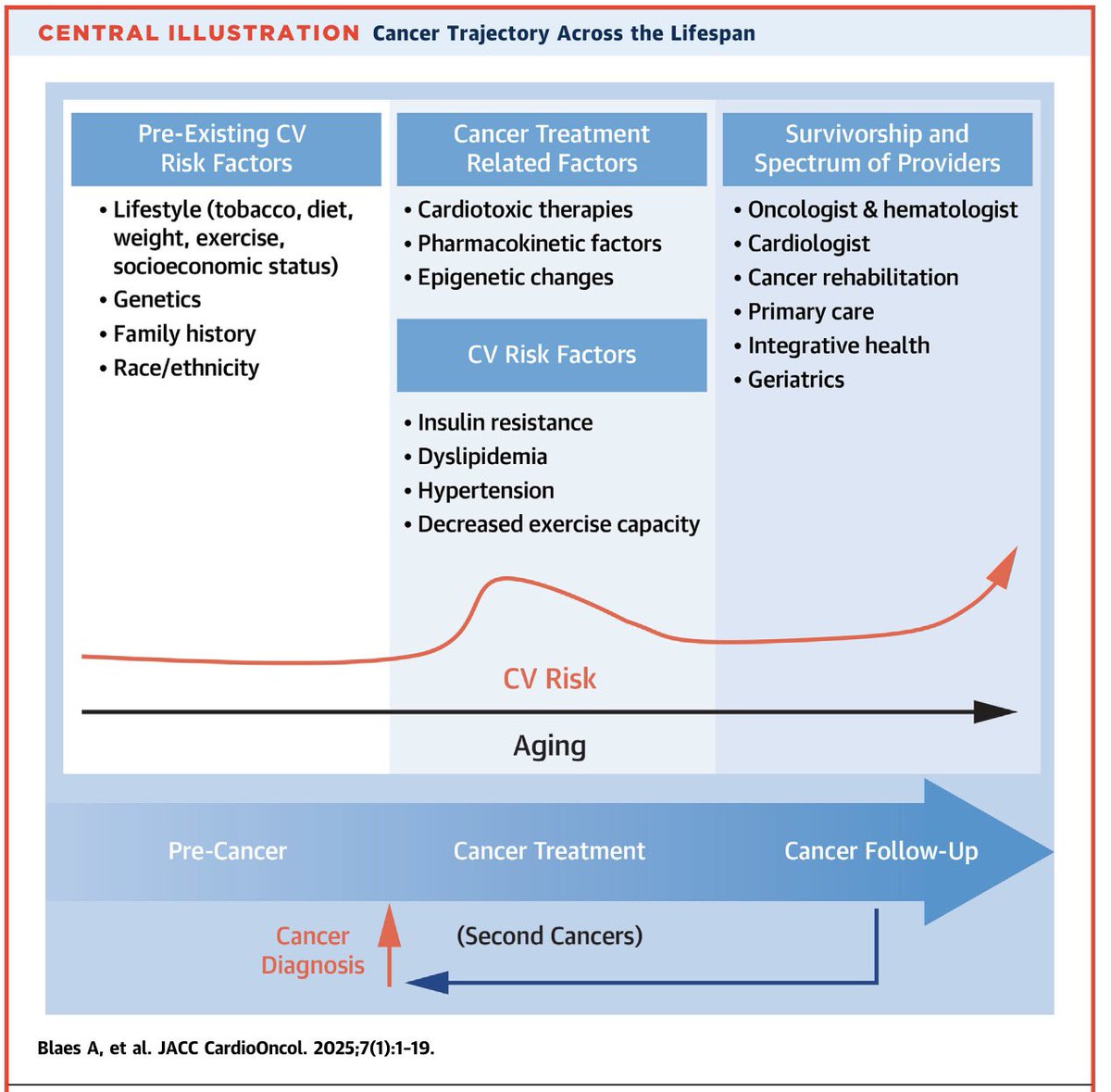
Cardiovascular considerations AFTER cancer therapy🫀
The final paper in a 3 part #JACCCardioOnc Expert Panel series exploring cardiovascular care before, during, & after cancer therapy
Cancer survivors remain at risk for future cardiovascular events throughout their lifespan.
Key contributors include:
🫀Pre-existing CV risk factors: Lifestyle, genetics, family history, race/ethnicity
🫀Cancer treatment-related factors:
📍Cardiotoxic therapies
📍Pharmacokinetic factors
📍Epigenetic changes
🫀Emerging CV risk factors
📍Insulin resistance
📍Dyslipidemia
📍Hypertension
📍Reduced exercise capacity
🫀Long-term survivorship requires a multidisciplinary approach involving oncologists, cardiologists, cancer rehabilitation, primary care physicians, & geriatrics.
Read more in @JACCJournals :
https://t.co/UZjR180Quh
#CardioOncology
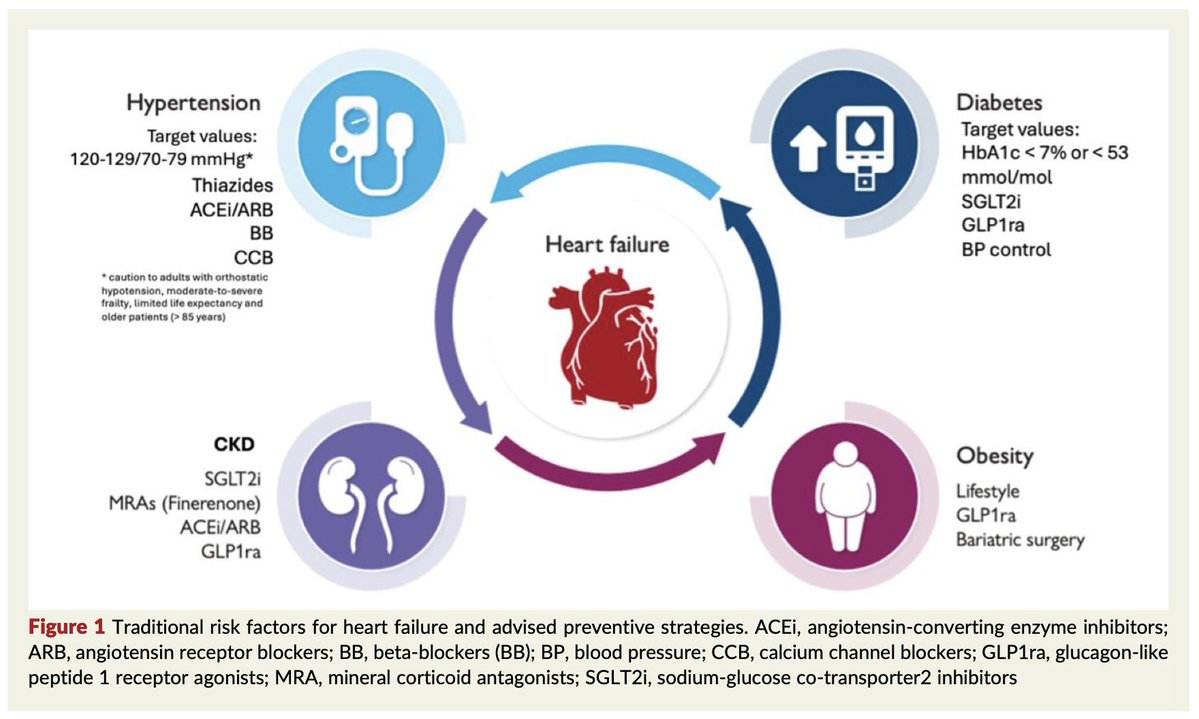
🫀What drives the development of heart failure?
The new #HFA_ESC scientific statement highlights the broad spectrum of risk factors contributing to #HeartFailure including:
📍Cardiac-kidney-metabolic syndrome
📍Lifestyle factors
📍Cancer therapies
📍Female-specific risk factors
📍Environmental & socioeconomic determinants
Preventing HF requires a holistic approach focused on early identification & management of these interconnected risks
Read more in #EJHF @EJHFEiC : https://t.co/EqOZ6zRLG7
@escardio@MarcoMetra@m4ggiesimpson
Cardiovascular considerations DURING cancer therapy🫀
The second of a 3 part #JACCCardioOnc Expert Panel series exploring cardiovascular care before, during, & after cancer therapy.
Recommendations for #CardioOncology care during cancer treatment:
Cardioprotection🛡️:
📍ACEI/ARB, beta-blockers, & statins may be considered to prevent ⬇️LVEF with anthracyclines 📍Consider dexrazoxane or liposomal doxorubicin for high cumulative anthracycline dose or LVEF <50% 📍Implement strategies to minimize cardiac radiation exposure
Surveillance🖥️:
📍Echo for anthracyclines & HER2-targeted therapies 📍Troponin & ECG for patients receiving ICIs
📍Prompt treatment & evaluation for high suspicion of ICI myocarditis 📍Blood pressure monitoring for VEGFi, BTKi, & ALKi therapies 📍Lipid monitoring for lorlatinib
Permissive cardiotoxicity⚖️:
📍Continue HER2-targeted therapy in selected patients with mild LV dysfunction, but need to evaluate risk & benefits 📍ACEi may be reasonable in patients with ⬆️ troponin during anthracycline therapy 📍Nitrates and/or calcium channel blockers can be considered to treat & rechallenge selected patients with 5-FU/capecitabine vasospasm, with close monitoring
Read more in @JACCJournals:
https://t.co/gxcpXpcDP2
Cardiovascular considerations BEFORE cancer therapy🫀
The first of a 3 part #JACCCardioOnc Expert Panel series exploring CV care before, during, & after cancer therapy.
🫀Goals of CV evaluation Prior to cancer therapy:
📍Identify and treat subclinical CVD and cardiovascular risk factors 📍Optimize management of pre-existing CVD and cardiovascular risk factors 📍Perform targeted risk assessment to help inform cancer treatment decisions 📍Establish baseline cardiovascular function 📍Optimize primary prevention therapies 📍Plan cardiovascular surveillance during treatment
🫀Current tools include clinical assessment, biomarkers, 12-lead ECG, #EchoFirst, & risk scores
🫀Important evidence gaps includes cardiotoxicity mechanisms, impact of pre-treatment CV evaluations on clinical outcomes, validation&implementation of risk scores, & the role of AI.
Read more in @jaccjournals: https://t.co/cTCY0Acg99
#CardioOncology
La PVC cambió de ser un indicador de HIPOVOLEMIA, a ser marcador de CONGESTIÓN VENOSA, en especial asociada a LRA. Usar volumen según la PVC, puede inducir paradójicamente congestión venosa…
https://t.co/pMz1sV0uRg
MINOCA: a structured pathway for optimal management!
Following diagnosis (ESC 2023 ACS), each patient is guided based on their endotype:
➡️ Reduced EF → early review 1-2 weeks
➡️ Preserved EF → review 4-6 weeks
➡️ Unconfirmed endotype → re-evaluation 7-14 days
#MINOCA
🚨Manejo contemporáneo de la Insuficiencia Cardíaca Aguda. 🫀💦
✔️La hospitalización ya no debe verse solo como una fase de “descongestión”, sino como una oportunidad para modificar la historia natural de la enfermedad. 🧐📈
✔️La ICA sigue asociándose a alta mortalidad y rehospitalización. El tiempo al tratamiento importa: reconocer y tratar temprano mejora desenlaces.
✔️BNP <100 o NT-proBNP <300 prácticamente descartan ICA.🔎
✔️El tratamiento inicial debe enfocarse en: O² si SatO₂ <90%, diuréticos IV tempranos, vasodilatadores IV si PAS >110 mmHg, identificar causas reversibles (SICA, arritmias, infección, valvulopatía, TEP, etc.).🎯
✔️La respuesta diurética debe evaluarse en las primeras 2 horas: diuresis >300 mL, Na urinario >70-80 mmol/L, si no se logra → duplicar dosis y considerar terapia secuencial.💦
✔️La hospitalización es el mejor momento para iniciar o intensificar tratamiento modificador de enfermedad (los 4 pilares ya!). 💊💊
📄🆓️⤵️ State-Of-The-Art Review 2026 @JACCJournals 👌🏻
https://t.co/xjS6PwznZu
https://t.co/CYXglmP4a5
Just published in JACC @JACCJournals!🫀
Acute HF care is evolving:
📍Rapid diagnosis
📍Early decongestion
📍Timely GDMT initiation
📍Structured follow-up
📍Focus on long-term outcomes, not just symptom relief
Grateful to have contributed to this international collaboration & learned so much from the exceptional experts involved in this work. Congratulations to @Jolie_Bruno_ and @AlexMebazaa for the leadership & to all co-authors on this important publication🫀
Read the full paper🔗: https://t.co/408QmNOznr
#HeartFailure #AcuteHeartFailure #JACC @jozinetm@BiykemB@GianluSava@pmyhre
@CorpusAlienumm Good save. Always follow the flowchart.
Mungkin di awal jika sudah on venti jika penolong > 2 orang bisa ada 1 yg handle dan take over manual BVM breathing nya 😊🙏🏽
B-lines are most often discussed in the context of pulmonary edema. But the spacing between them carries a different kind of information — one that reflects structural lung disease rather than fluid overload.