Emergency medicine is a team sport.
If you’re the morning doc, your job is to help the night doc get home; your job is NOT to repeatedly question and second guess the night doc’s decision making.
@ChuckWurster ... All staff entered the facility thru a dedicated “clean” entrance and were screened for symptoms prior to being allowed to move to their respective departments. 2/2
@ChuckWurster During SARS in 2003 in southern Ontario, we wore full PPE for every patient, changing gloves between patients. Eight hours in an N95 was a tiring respiratory experience. Surgical mask may have been adequate but we didn’t know any better at the time. 1/2
@e_med_doc@usamabasit You’ll never go back! Casino shifts saved my life and extended my career. No more feeling like dozing off at traffic lights on my way home. Recovery time reduced from 3 days to 1
Do combined ultrasound and electrocardiogram-rhythm findings predict survival in emergency department cardiac arrest patients? The Second Sonography in Hypotension and Cardiac Arrest in the Emergency Department (SHoC-ED2) study. https://t.co/pBoo7sTjg1
Peritonsillar Abscess telescopic submandibular AND endocavitary views for comparison!
ED team aspirated 6+ satisfying mL's and discharged.
Learn the submandibular technique starring @aliteplo thanks to @mghedus :
https://t.co/dtRuXWGU4u
#POCUS#FOAMed
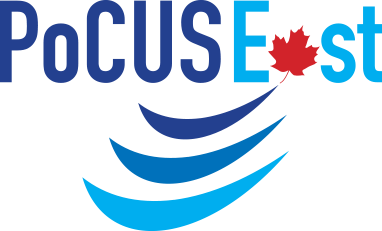
New Trick of Trade: Recent chats on linear U/S probe in peripheral IV placement & tegaderm damaging probe.
Slide probe into folded “cuff” of sterile glove. Flat edge and no wrinkles with probe cover. Bonus: Glove 🤚 fingers out of way. (Gel goes in first).
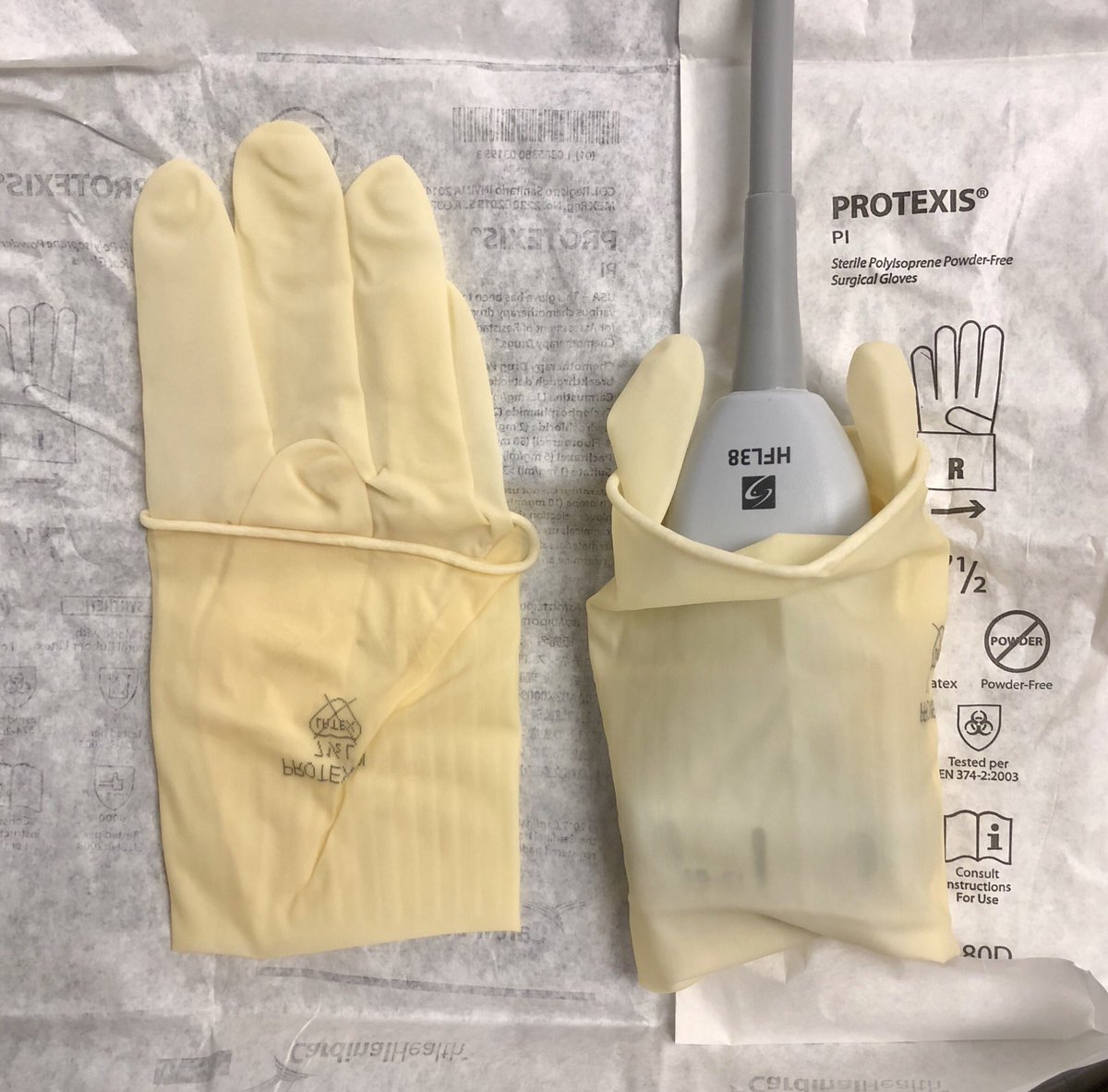
Great to here @TRRBB in her hometown answer the question is pocus a reliable predictor of outcome during atraumatic, non-shockable cardiac arrest at #CAEP19 Next stop @ELalandeEM at #ICEM2019@NetworkShoc @eccucourse https://t.co/7DxG3FggOk @emergmedottawa