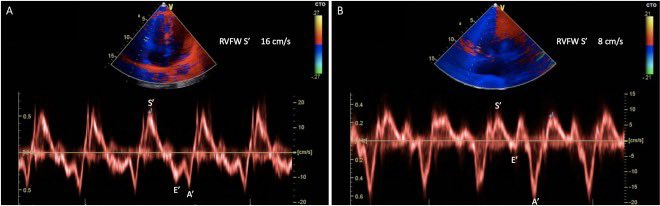
The right ventricle (RV) contracts mostly (70%) in the longitudinal direction.
Using tissue Doppler (i.e. hitting the TDI and then PWD buttons), S' represents the velocity of the lateral tricuspid annulus during systole.
S’ < 9.5 cm/s suggests RV systolic dysfunction.
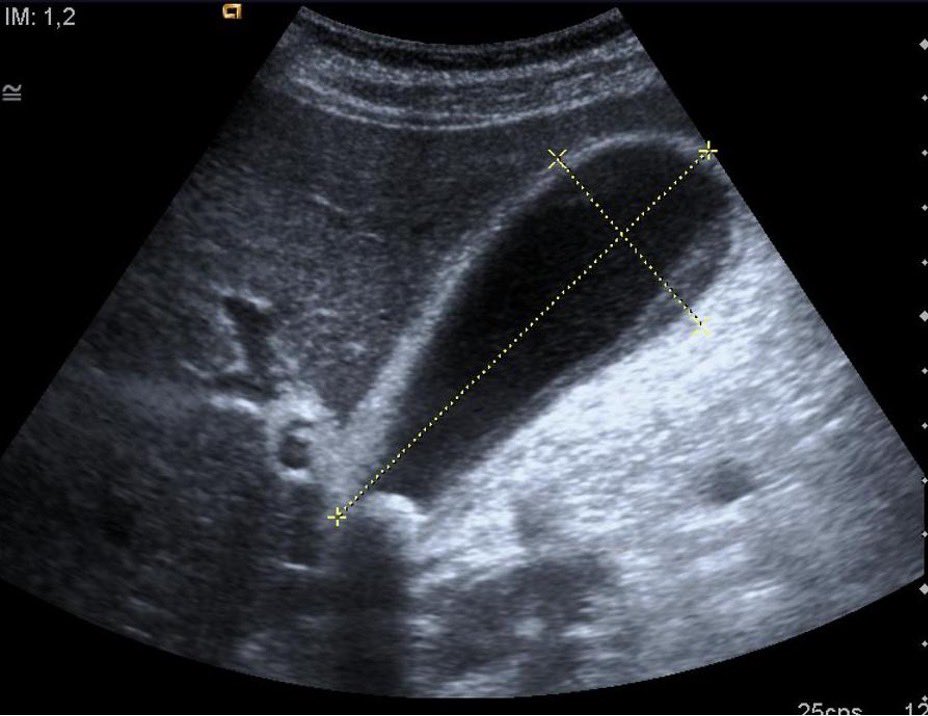
Gallbladder hydrops: size of GB > 4 cm (transverse) x > 9 cm (longitudinal)
• Most commonly caused by impacted gallstones (at neck)
• Prolonged blockage of cystic duct leads to increased intraluminal pressure, inflammation
> High suspicion of cholecystitis (surgery consult)
A POCUS Echo Pearl by Rutgers alum @RobertAdrianMD
The descending aorta can guide effusion identification. Pericardial effusions are anterior to the descending aorta, while left pleural effusions are posterior to it in the parasternal long axis view.
Hot tips for Ocular POCUS by @cooperali
- Use cold gel, it has more structural integrity to minimize applied pressure
- Brace scanning hand on patient's forehead to minimize pressure to globe
- “Ocular” setting is lower energy, minimizes potential damage to corneal epithelium
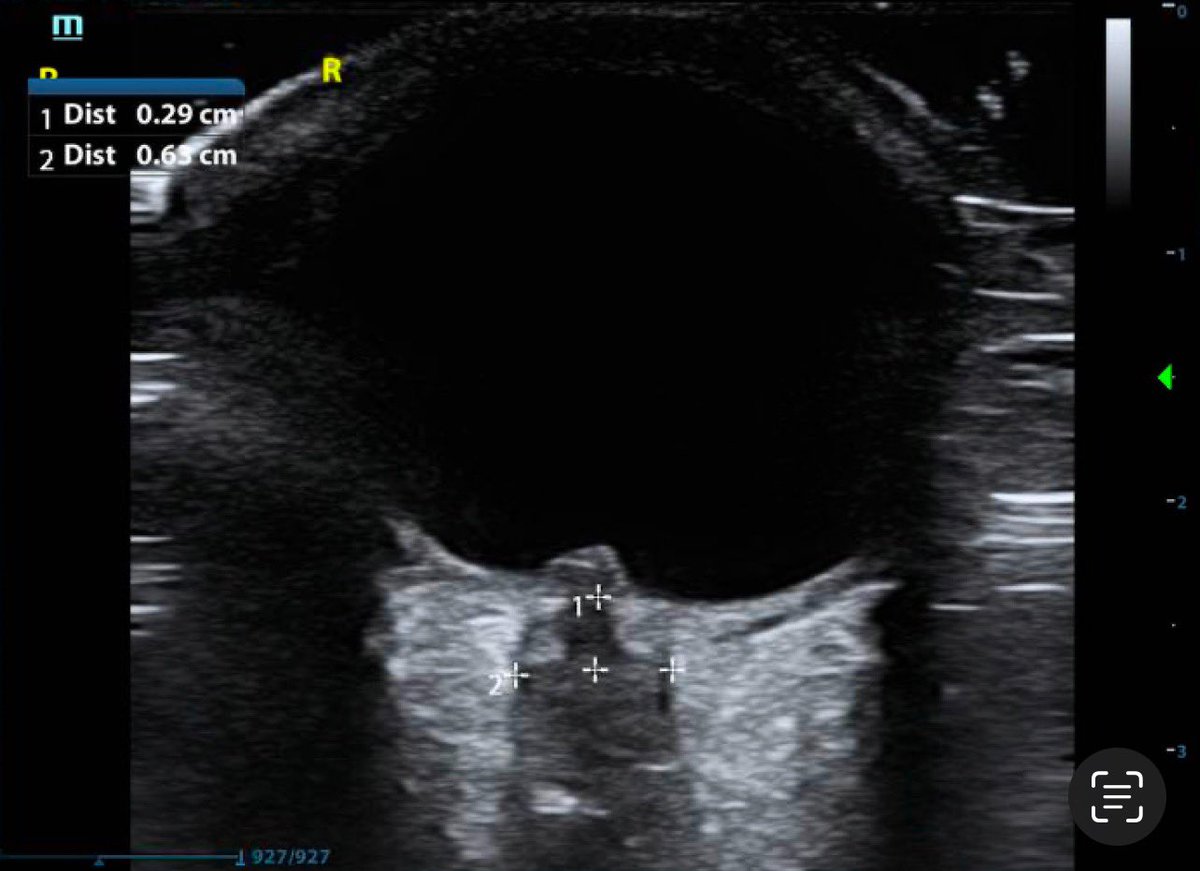
Differentiating Lymph Nodes and Abscesses by POCUS:
- Abscess: typically anechoic or mixed echogenicity, irregular contours and the appropriately named “squish sign”
- Lymph node: well-circumscribed, typically a hyperechoic hilum is protruding into the hypoechoic core (see image)
POCUS guidance in thoracentesis helps decrease the risk of complications like pneumothorax, intra-abd or vasc injury:
Identify biggest pocket superior to most cephalad position of expirational diaphragm and determine depth to reach pleural fluid and max permissible depth.
ET tube confirmation by POCUS:
- Bullet sign: reverberation artifact in trachea, single air-mucosal interface = tracheal intubation
- Double tract sign: two air mucosal interfaces with posterior shadowing = esophageal intubation
Dynamic air bronchograms (hyperechoic lines, moving within consolidated lung throughout resp cycle) are an ultrasonographic sign of pneumonia
• Artifact due to air in bronchioles surrounded by consolidated lung
• Up to 94% specificity in differentiating pneumonia vs atelectasis
DO-IT-YOURSELF PHANTOM MODELS for ultrasound guided IV placement: go to https://t.co/v07R4DaFBl for a step-by-step guide created by our resident @PeterAlsharif
Evaluating for nephrolithiasis using POCUS usually entails assessing for the secondary finding of hydronephrosis.
Try also looking for the primary finding (i.e. the stone itself) in the ureterovesicular junction, which is the most common site of obstruction.
With a shallow object of interest (e.g. ?foreign body in finger or toe), use an ultrasound water bath to:
1) avoid distorting the object via direct pressure from the probe.
2) bring the object within the focal zone in center of the screen where imaging resolution is best.
Free fluid is gravitationally dependent. Therefore, placing the patient in Trendelenburg (i.e. head declined below feet) when performing the FAST exam will increase sensitivity for detecting free fluid in Morrison's pouch.
A right heart thrombus is thin, mobile, and worm-like. It floats to-and-fro within the right-sided chambers.
A vegetation attaches to the valve, usually the proximal side. Its movement is usually chaotic and independent from that of the valve (though not in this case).
Replacing a G-tube is quick if not out too long and no trauma.
Yet, confirmation by gastrograffin x-ray takes forever.
Consider POCUS to confirm placement:
- Place probe adjacent to tube, see catheter and balloon
- Instill 50+ cc of saline, watch stomach expand with bubbles
Evidence suggests that POCUS is superior to the landmark technique for accurately identifying the Cricothyroid Membrane. This may be useful for marking the CTM prior to a difficult anticipated airway (i.e. an obese hypercarbic COPD or opioid intox patient).
How to measure AAA diameter correctly?
- measure outer wall to outer wall, at the widest diameter
- avoid underestimation by only measuring the lumen, always include thrombus / plaque