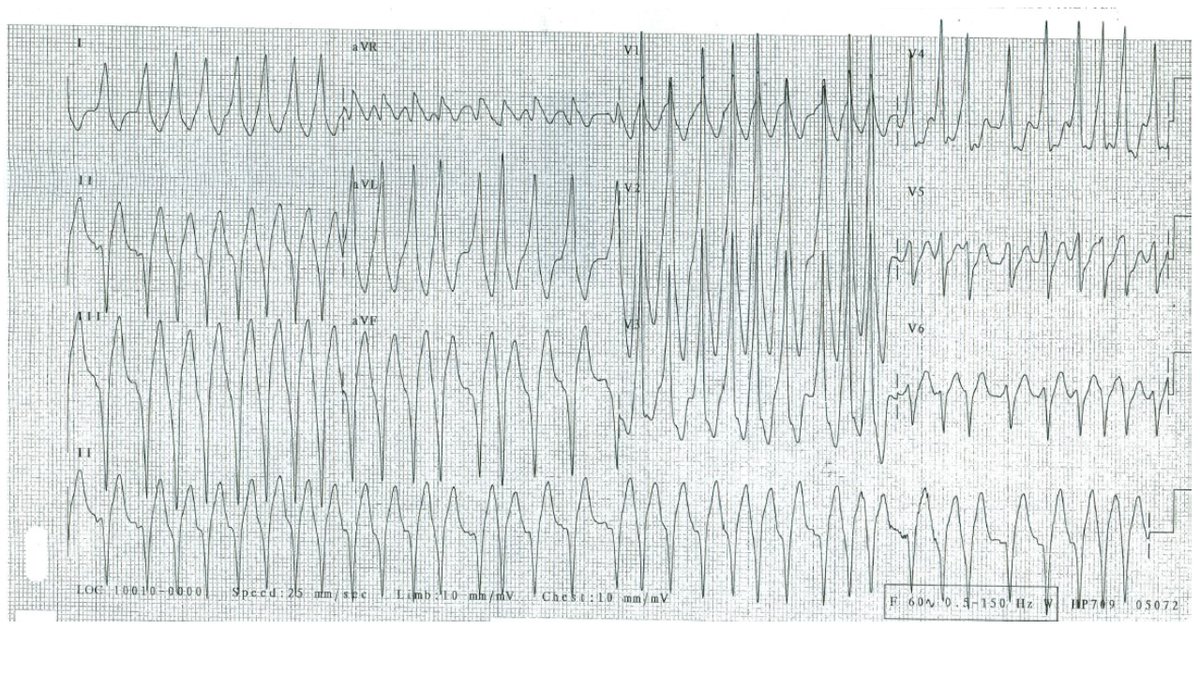
@supadhyaymd@GeorgeBodziock@WFCardiology Great thoughts - totally agree. WCT transitions into slightly faster NCT. DDx includes VT initiating PSVT vs SVT with aberrancy that then peels back, narrows, and speeds up. If its all SVT, tachycardia getting faster with resolution of BBB strongly suggests ORT (Coumel's sign).
@WFCardiology@GeorgeBodziock Thanks for the responses! I thought a nice example of rate dependent LBBB (sinus rate slows slightly antecedent to QRS narrowing) giving us a look at T-wave changes due to memory. First described by Dr. Kanu Chatterjee in 1969!
@GangoliBorun@GeorgeBodziock@WFCardiology The ECG was read as AF (which is why she was referred to EP). P-waves are seen (ruling out AF) but the p-waves are not responsible for most of the narrow QRS complexes. The most likely diagnosis for this irregular narrow complex rhythm is an accelerated junctional rhythm.
@Van_Lav@GeorgeBodziock@WFCardiology Agree -- its not AF because there are clearly p-waves. But the p-wave before the 5th complex would not have time to create the QRS. So a diagnosis of junctional rhythm makes the most sense. Her Holter is shown here - incessant arrhythmia is noted.
@GeorgeBodziock@WFCardiology@DocBanks84 + delta wave in V1 indicates L sided AP (initial forces are toward V1, an anterior chest lead - this means that ventricular activation starts posterior [mitral annulus]). Will be important to counsel the patient that trans-septal or retroaortic mapping/ablation will be required.
@GeorgeBodziock@WFCardiology You got it @DocBanks84 !
With pre-excited AF, you can do:
1. DCCV
2. procainamide
3. amiodarone
Need to avoid BB/CCB/adenosine.
Location of the AP based on this ECG? This will help you counsel the patient about risks of ablation.
@GeorgeBodziock@WFCardiology After the V-A-V response, the tachycardia continues. This rules out AT. The longer VA time during ATP as compared to the VA time during tachycardia suggests that the A and V are activated in parallel and not in series. In sum, this is most consistent with typical AVNRT.
Device EGMs from recent admit to hospital in a patient with CRT-D. Thoughts on DDx and likeliest rhythm diagnosis for the tachycardia? First EGM slide is immediately preceding second EGM slide.
@GeorgeBodziock@WFCardiology The end of the 1st panel (and into the 2nd) shows the device initiating ATP. The ventricular anti-tachycardia pacing advances the atrial rate to the rate of ventricular pacing, with a longer VA time than what was seen during tachycardia. When ATP is released, we see a V-A-V respo
@GeorgeBodziock@WFCardiology Nice answers!First panel shows a tachycardia with a 1:1 A:V relationship. V-A time is very short, making VT with 1:1 retrograde conduction (or ORT) unlikely but not impossible. AT is possible, although the consistent VA time (VA linking) makes this less likely.Likeliest is AVNRT.
@GeorgeBodziock@WFCardiology Nice observation that QRS morphology varies, which is likely due to subtle differences in depolarization between the junctional beats and the conducted beats.
@GeorgeBodziock@WFCardiology Nice responses! My interpretation was: Accelerated junctional rhythm with JA conduction (P-waves are low-high ruling out sinus rhythm) which likely transitions from retroFast to retroSlow with the retroSlow beat echoing antegrade down the fast pathway.