Jürgen Klinsmann: “There were 70,000 people, we were warming up seriously. While ‘Live Is Life’ was playing, Maradona started juggling the ball. We stopped warming up, because there was nothing more we could do except watch him.”
Castell Harlech has watched over this landscape for 700+ years. Built by Edward I, it has endured rebellion, siege and shifting tides—now overlooking Royal St David’s, where the game unfolds beneath its shadow.
🫀 Myocardial perfusion imaging (MPI) is routinely used to assess ischaemia in CTO patients—but does it actually predict outcomes after PCI?
This large registry study provides an important answer.
✨ Study at a glance:
🔹 319 patients undergoing CTO-PCI
🔹 65% had moderate–severe ischaemia (≥10% LV)
🔹 Follow-up: 90 days + 5 years
✨ Key findings:
🔹 No difference in hard outcomes between groups:
➡️ all-cause mortality
➡️ MACCE (MI, stroke, HF, CV death)
🔹 At both 90 days and 5 years:
👉 ischaemia burden did NOT predict prognosis
📊 But here’s the nuance:
🔹 Patients with higher ischaemic burden had:
➡️ lower risk of angina hospitalisation at 5 years
👉 Suggesting a greater symptomatic benefit from CTO-PCI
⚠️ Important considerations:
👉 Ischaemia defined globally (≥10% LV), not vessel-specific
👉 Mix of SPECT and PET imaging
👉 No comparison with medical therapy alone
💡 Clinical take-home message:
👉 Ischaemia is not a prognostic marker after CTO-PCI
👉 But it may help identify patients:
✔ more likely to benefit symptomatically
✔ with greater improvement in quality of life
🧠 This reinforces a growing concept:
👉 CTO-PCI should be:
symptom-driven, not ischaemia-driven
👉 Imaging should guide selection—but not dictate it
🚨 Bottom line:
More ischaemia ≠ better outcomes—only better symptom relief.
#Cardiology #CTO #PCI #Ischaemia #CardiacImaging #PET #SPECT #CoronaryArteryDisease #InterventionalCardiology #QualityOfLife 🫀📊
I was up last night with a STEMI until 4:30. For my entire career I’ve gone to work the next day with whatever sleep I could get. Not anymore. Today, I slept in and did chart work from home. You can’t fly an airplane or drive a truck if you’ve been up all night. Why should it be different for docs?
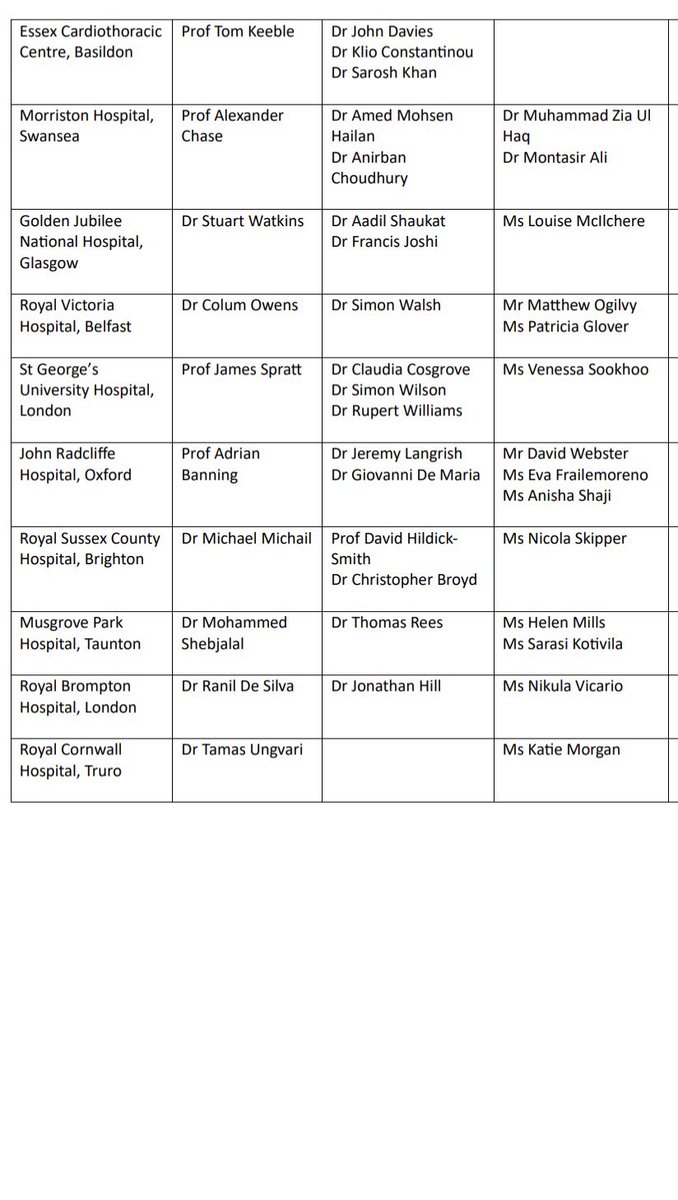
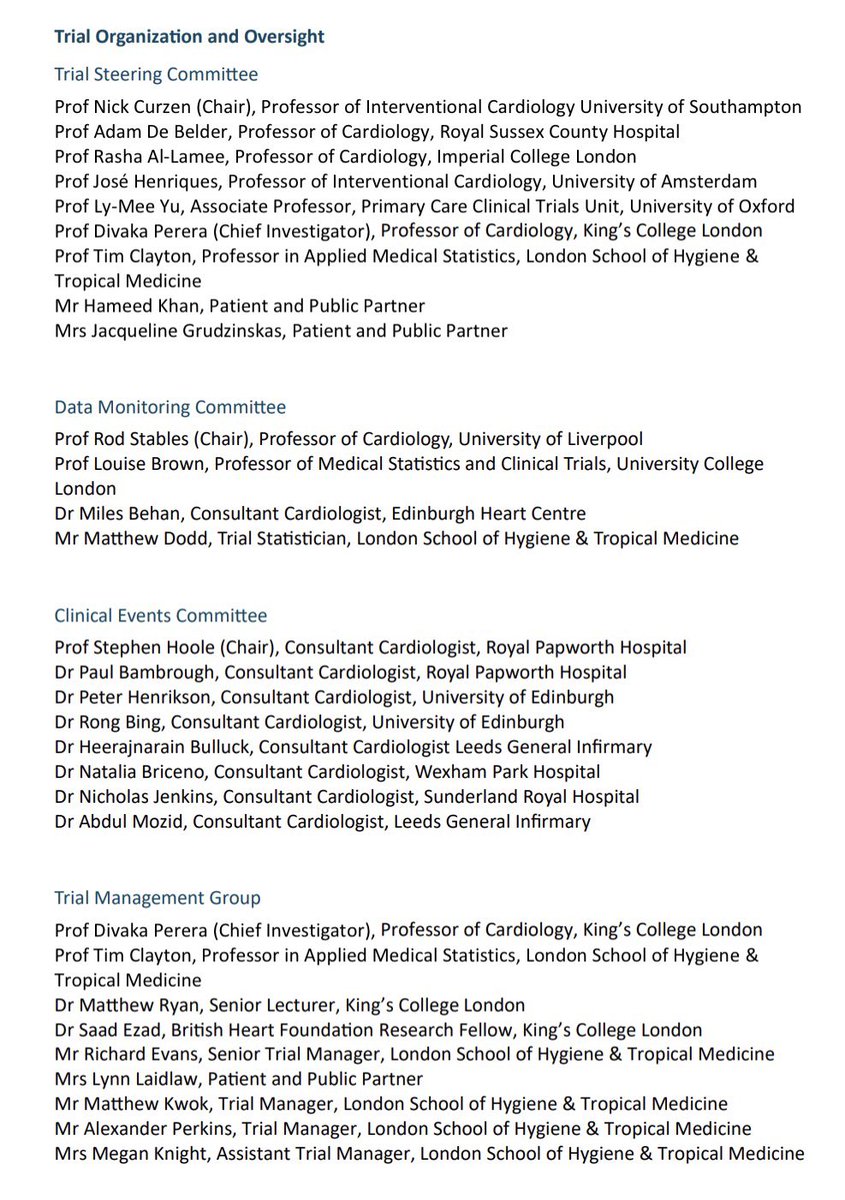
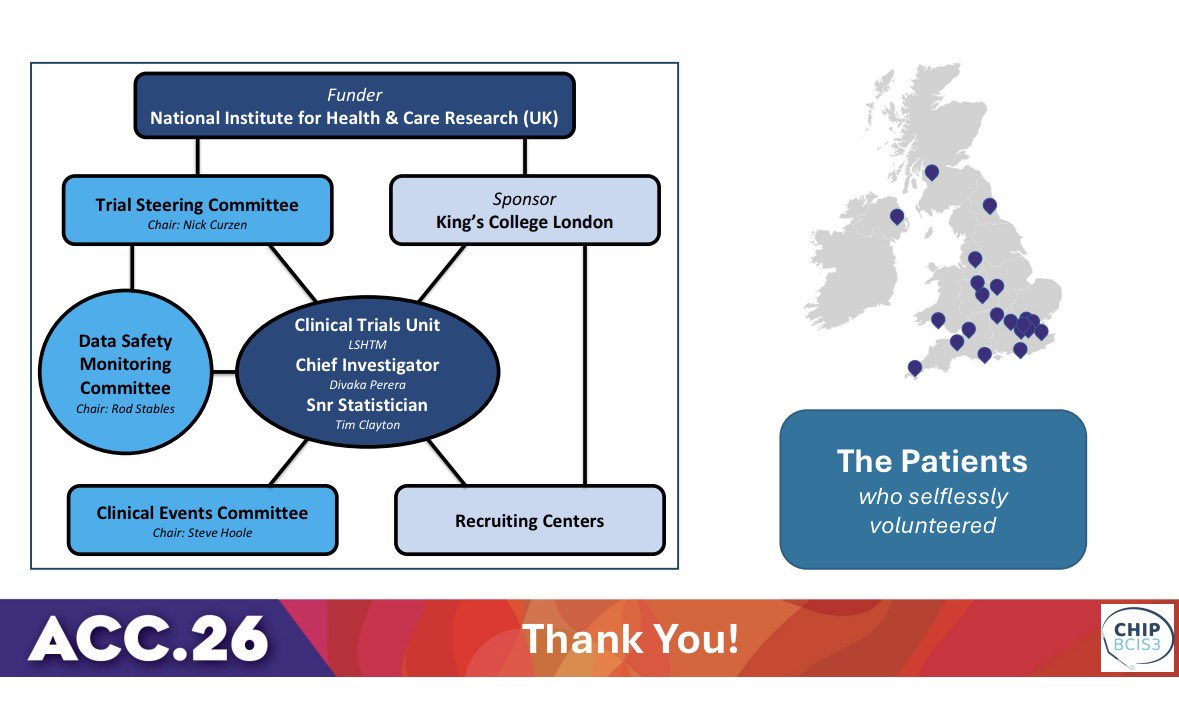
This remarkable project would not have been possible if not for the dedication and sacrifices made by many.
The investigators are indebted to the 300 patients who selflessly volunteered and to those who worked tirelessly behind the scenes.
🙏🏽
UFH-STEMI trial: In STEMI patients undergoing primary PCI, pretreatment with UFH 70-100 IU/kg at prehospital first medical contact improved infarct-related artery patency without increasing the risk of BARC types 3-5 bleeding. #ACC26 View slides here: https://t.co/aEoDpNUpiE
Congratulations to @divaka_perera & the team …. Important message to interventionists who have allowed non evidence based intuition to influence their choice of impella in high risk pci!? It does not improve patient outcomes
@djc795 A) you have to count procedural bleeding
B) Antiplatelets are not nothing (AVERROES and BAFTA)
C) Apixaban is really good
Also…I wonder if a real world analysis ever found higher bleeding w LAAC would such a study get published
@AndrewFoy82@MRuzieh
BRITISH addresses a key question in this field…. Will effect guidelines whether scar is an arbiter of ICD mortality benefit or not @drflett. A chance for UK cardiology to make a difference!