@jon_bailey_anes@glauncel@doctimcook Yes agree lots of ways to train bronch skills. Disagree that the topicalization easy to do (well) or teach. We’ve benefited from having worldwide airway experts train us. Most of the AFOI gone sideways I’ve seen are from oversedation to compensate for poor topicalization.
@glauncel@doctimcook Agree Gord. The topicalization technique is the key learning. Asleep fibrotic can train the bronch skills, probably harder than AFOI from a bronch management perspective.
@DerrickArthor@RyanMarino@Rusticus17761 I use sufentanil (10x potency of fentanyl) on a daily basis in OR. I’ve spilled it on my hands many times over the years: nothing happens. Also had remifenanil (a powder) vials break and go on my hands: nothing happens. It’s all a charade.
@msenussiMD Or just use some gauze and compress the vein between the various steps. Not sure the need to reinvent the wheel. On board with the excellent US needle viz tho!
@OBsleepmerchant If only it was a sophisticated as that. I doubt many in ICUs know the T1/2 of commonly used NMB. Every shift I work I make an effort to teach folks that TOF isn’t out of 4. Most think 4/4 = full recovery.
@jwnickerson@CanadasLifeline I’d be happy to be allowed to donate. Canadian Blood Service don’t seem to understand that people in England donate and receive blood without CJD. I’m English so I can’t donate. I’m also O (-)
1/16
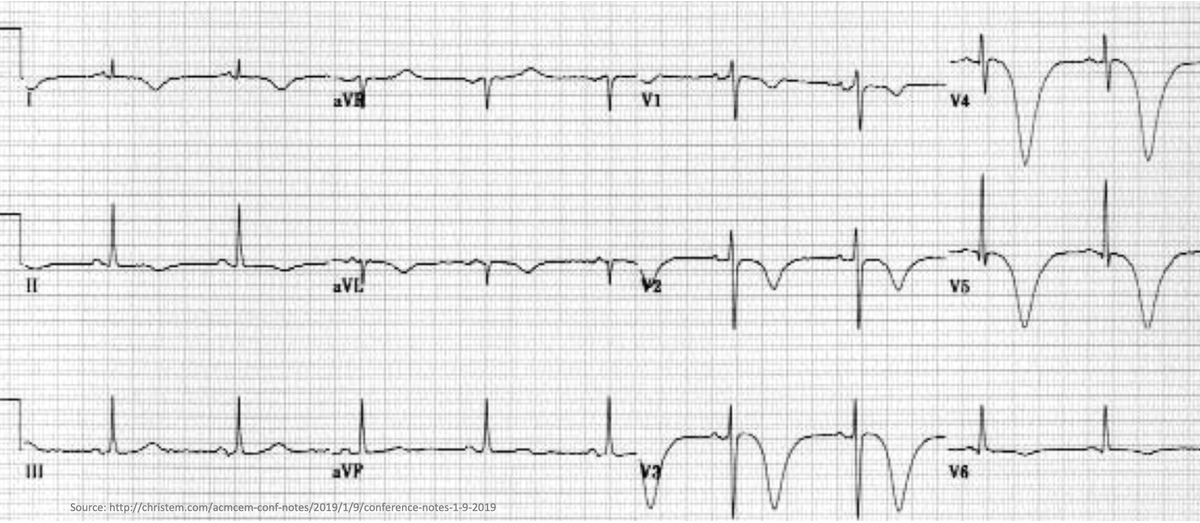
🤔Why does subarachnoid hemorrhage lead to deep/inverted "cerebral T-waves"?
This ECG finding is so dramatic. But as we will see, these patients often have normal hearts.
Why does an issue in the brain manifest on a test of the heart?
@OBsleepmerchant Yes. CAS required monitor of equal importance to Spo2 or capnography. Yet as a specialty we are sloppy with how we use it. We should leave the NMJ as we found it. IMO with the drugs and quantTOF monitors we have available, there is zero excuse for residual NMB. Rates should = 0%
Time to move on. We eventually stopped using halothane because we got better drugs. Neo still works ok if you use it right, but so does halothane, Pentothal, etc etc. We have a better drug now.
In a multicenter matched cohort analysis, sugammadex administration was associated with a 30% reduced risk of pulmonary complications, a 47% reduced risk of pneumonia, and a 55% reduced risk of respiratory failure compared to neostigmine. https://t.co/rGDuJ636en
@OBsleepmerchant Yep. As with all drugs, there are reasons to avoid. I’m totally on board with quantitative TOF and appropriate dosing of neo. It works very well under those circumstances. I would argue that our current rates of residual neuromuscular block are higher than 1 + 2 combined.
@garrettsbarry@bmacaulay2000@AnesthesiaCons1@NicholasChrimes Yeah exactly. I used neo regularly with quantitative TOF and just ensure they are actually >0.9 before extubating. Many just “wing it” unfortunately. Sug let’s them get away with poor monitoring more, which makes it a safer drug IMO. But quantitative TOF is really the 🔑 👌🏻
@glauncel Agree. I’m more concerned with the rates of residual neuromuscular block in PACU, which I fix with sugammadex on a regular basis while on call. Those rates are 30-40% w/ neo and w/o quantitative monitoring. Neo is still an effective drug if used correctly, but often isn’t.
In a multicenter matched cohort analysis, sugammadex administration was associated with a 30% reduced risk of pulmonary complications, a 47% reduced risk of pneumonia, and a 55% reduced risk of respiratory failure compared to neostigmine. https://t.co/rGDuJ636en