🏆Best RTT Paper Award at #ESTRO25!
Can #APRTs improve workflow + cut costs in online #adaptiveRT?
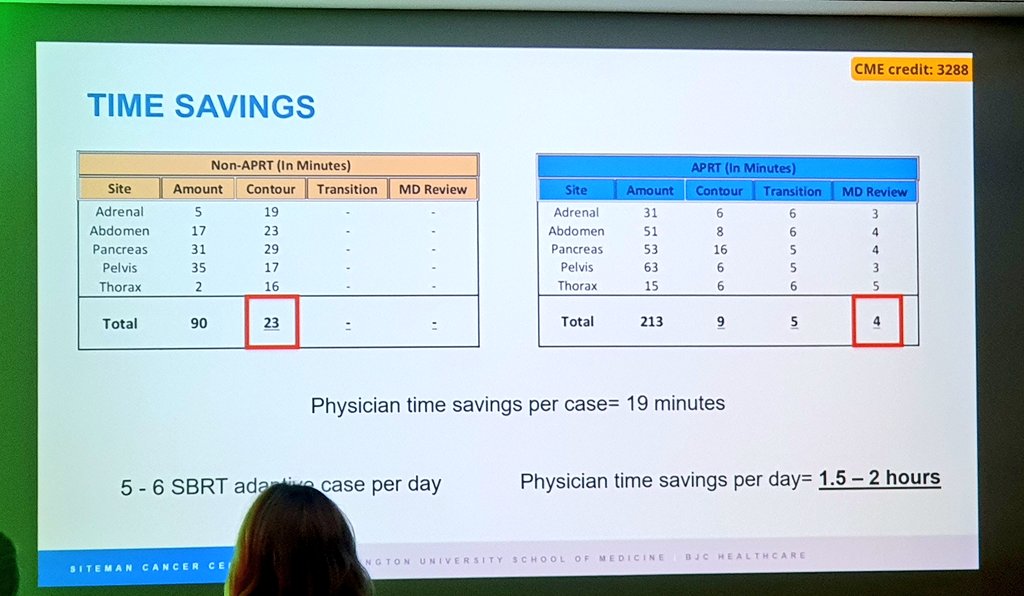
This study shows APRT-led contouring saves time ⏱️ & money 💰vs. RO-led teams.
Redefining roles = better care & new #RTT careers.
👉 https://t.co/rnjjemZB3v
#Radiotherapy
@SameerKeoleMD@ASTRO_org@RobAPRT has paved the way for this role in the US and has published on implementing his role as an APRT for adaptive contouring
https://t.co/YF1SMQI2bO
He also recently presented an award winning abstract that time savings -> cost savings
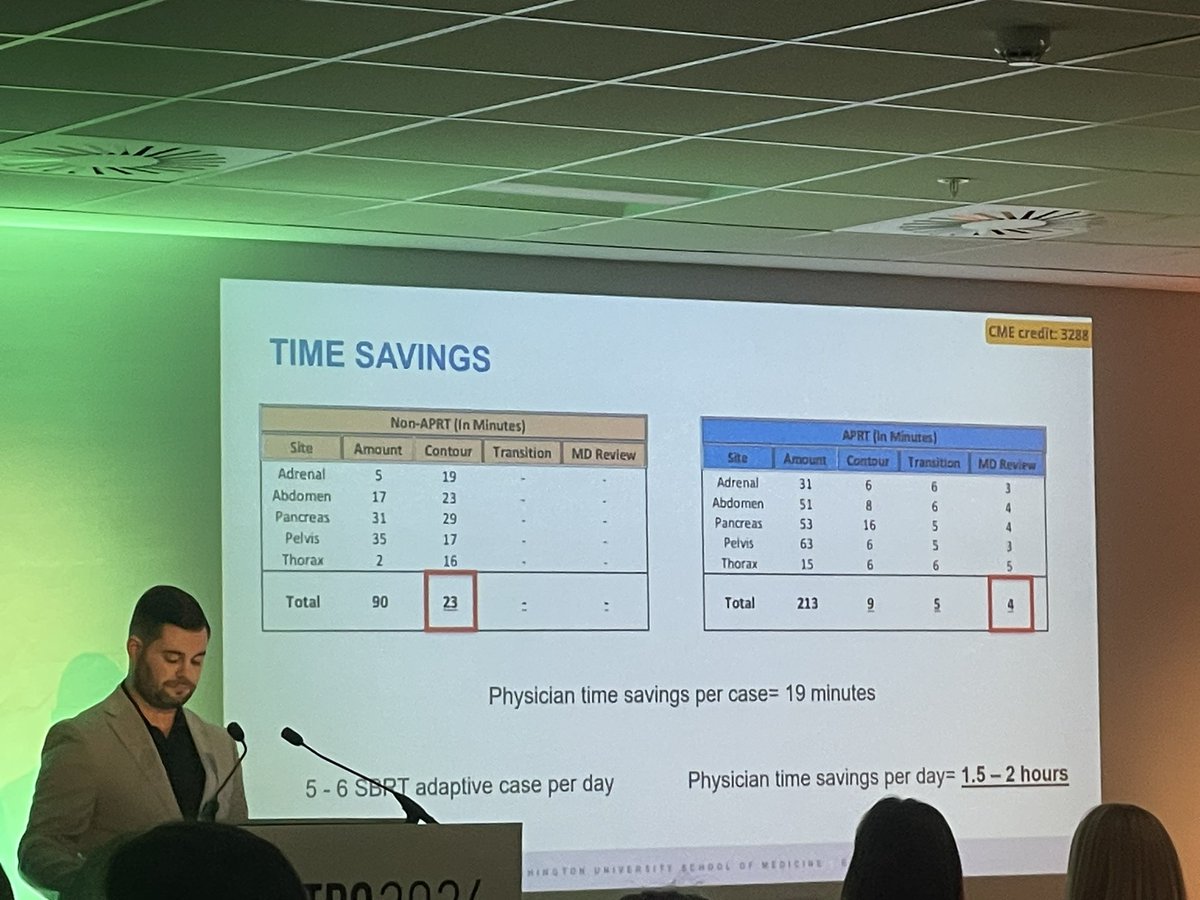
@WashUMedRadOnc adaptive APRT @RobAPRT presenting in the #ESTRO25 plenary hall his award winning work on demonstrating the financial savings of implementing an adaptive APRT in a busy ART clinic ☢️
In addition to winning BEST PAPER submitted to RTT track for #ESTRO25 🎉 @RobAPRT will be presenting this work - May 5, 11:40am Vienna time
"APRT Analysis for Online Adaptive Radiotherapy Contouring and Adaptor Model Evaluations Using Time-Driven Activity-Based Costing" #radonc
Final speaker in our SEALs adaptive and AI program- Robbie Beckert from
Wash U is speaking about “Utilization of an APRR for Online Adaptive Radiotherapy”. We appreciate the knowledge sharing from the adaptive therapy speakers! #ACRO2025@ACRORadOnc@ACROresident
Congrats to @RobAPRT! 👏His paper "APRT Analysis for Online Adaptive Radiotherapy Contouring & Adaptor Model Evaluations Using Time-Driven Activity-Based Costing" has been awarded BEST PAPER submitted to RT track @ESTRO_RT! He will present in Vienna in May #ESTRO25.
Thrilled to see this Adaptive White paper in print @IJROBP - This was a labor of love from start to finish by all members of this Task Force, & a delight to co-chair w/ Indrin. Thank you @ASTRO_org for helping to organize the best of our work!
https://t.co/kcg8S4s8fV
Strong work @AllenMoMDPhD and team for successfully creating and implementing this workflow on the PARTy trial. Fantastic treatment option for patients with pelvic disease and prior radiation!
First patient treated on our adaptive proton trial today❗ Thank you to this patient and Drs. Zhang, Liu, Zhao, Kim, Perkins and the rest of the adaptive radiation team @WashURadOnc for making this happen! @SitemanCenter#adaptiveRT#radonc
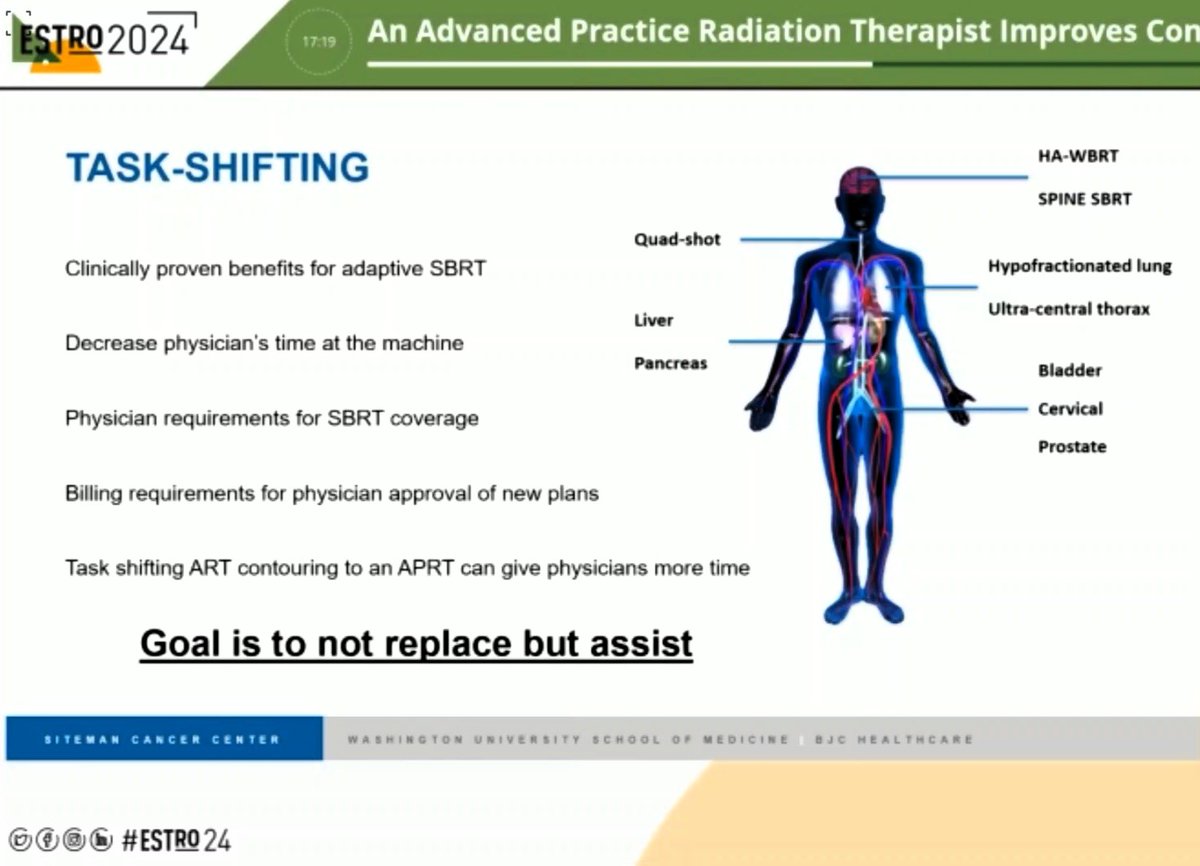
Very grateful to have presented at #ESTRO2024 on how an Advanced Practice Radiation Therapist, specialized in online adaptive radiotherapy contouring, reduced contouring times while also allowing physician more time to conduct work only they can do
#APRT#AdaptiveRT#RadOnc#USA
Last week, Cliff Robinson, MD received a 2024 @WUSTLmed Dean’s Impact Award!🙌 This award recognizes faculty who have demonstrated enduring commitment to advancing the careers of others thru exceptional mentorship or sponsorship - sounds like @SBRT_CR! So lucky to have him here!
Congrats to @RobAPRT who presented our @WashURadOnc data on the training and implementation of an APRT specializing in CBCT-guided online adaptive radiotherapy contouring at #ESTRO2024 ☢️
Not trying to set off the workforce anxiety train, but that doesn’t really apply here though. Adaptive adds considerable NEW time so an APRT can partially offset this, not fully.
Remember that in current state there are no adaptive codes, so this literally is largely non reimbursed physician time. Shifting it to qualified staff is win win so the radonc can see new patients. It’s sort of like saying a brachy doc should personally sterilize everything they use to not reduce work for the doc.
We are recruiting for 2 more positions so volume is great here. 2030 is right around the corner so perhaps this largely applies outside the Midwest where I have seen so many jobs open since I moved to Ohio. I think most docs would rather be well supported and busy doing what they enjoy then seeing fewer patients with minimal support.
Perhaps another way to look at it…Should residency slots close if people use scribes? Or Dragon to dictate? Or places that use AI powered clinic note writers? Just trying to follow the logic. There are so many better reasons to close slots (ie lack good comprehensive training…residency is to train in everything so you can bring the latest to your practice) other than supporting your physicians and residents to focus on their value add.
Perhaps I am crazy 🤪 I have tried since med school to improve efficiency and get closer to doctoring and less scut.
Again, not challenging workforces stats. Simply saying providing physicians with support to do their jobs is not a bad thing. This is very different from having APPs run a fully independent clinic and sign RT plans and see OTVs all on their own.
Pioneering data on radiographer-led online adaptive RT from @WashURadOnc masterfully presented by @RobAPRT
So lucky to have 1 of only 2 x APRTs in the US here at #ESTRO24!
Powerful data for both adaptive RT & expanding interdisciplinary roles in radiotherapy!
We are 1st in the US to successfully implement an Advanced Practice Rad Therapist (APRT), specialized in online adaptive radiation therapy (oART) contouring into our high-volume clinic! We are proud to have @RobAPRT presenting his findings at #ESTRO24