'Twice, my family came to say goodbye. Now I’m driving again'.
Physios are giving stroke patients like David their lives back.
Rehabilitation should be accessible to everyone who needs it for as long as they need it.
#RightToRehab
if a young person is detached from work at nineteen, they’ll still be detached at twenty-nine.
Milburn’s review matters and the fact it is a rehash, makes it matter even more. https://t.co/ZNiUFYBImd
Productivity gains aren’t always cash-releasing.
If AI saves clinician’s time, demand will expand to consume it...
More patients seen.
More conditions identified.
More follow-up generated.
More costs…
… expectations rise.
The NHS is a demand sponge. https://t.co/GRzK0HYNsf
job losses on this scale?
The biggest number previously?
British Airways; 12,000 job-cuts in April 2020.
The NHS is set to lose 18,000.a survey found 47% of Trusts were cutting services 37% were cutting clinical posts. https://t.co/0F7R9MX6th
‘Advanced practice physiotherapists are highly trained, regulated practitioners who provide expert care to patients in a range of settings across the NHS.
‘Their skills, knowledge and expertise complement what other professions bring to teams treating patients and have an exceptionally strong record on safety.'
The CSP has responded strongly to media claims over the weekend around the safety of advanced practice roles in the NHS.
Read more: https://t.co/wnQtmJ4OUH
More people are surviving strokes than ever before in the UK.
But their hopes of getting better are being dashed because of a lack of physiotherapists.
We highlight critical workforce shortages with @ACPIN_UK and @TheStrokeAssoc.
#RightToRehab
https://t.co/8AiVpLKbh7
BLOG What does dementia rehabilitation mean to us as AHPs ? ‘Podiatry for people with dementia focuses on maintaining mobility and independence by encouraging and helping to maintain a healthy active lifestyle through good foot health’ https://t.co/iAYEr9MAWo… @alzscot
⭐ The duty of candour matters.
Health and care professionals must be open and honest, especially when things go wrong. It’s not just good practice, it’s a professional duty that builds trust and safeguards patients.
Read more on our website 👉 https://t.co/7MKBxWjcyF
@LucyyMacKinnon@ExplosiveEnema2 Yes we should compare like with like in roles eg a consultant clinical scientist in genetics with 12 years PG education a doctorate, fellow of RC of Pathology is on AfC band 8c £76k, £30k less than medical colleagues
Are we realising the potential of our networks to make change happen?
Most innovation emerges from collaborative projects where teams openly “borrow” & adapt each other’s (often small but powerful) ideas. Many networks & communities of practice could achieve so much more by experimenting together around collective priorities to generate & share new solutions.
This is beyond spreading known “best” or “good” practices. It is about innovating to design new solutions collectively.
So I appreciated this piece from Ed Morrison of @Strategic_Doing about three different kinds of networks:
- Advocacy networks are communities that seek to mobilise people, creating pressure to shift policies, priorities or messages in a particular direction. Their aim is to connect & influence rather than to change how they themselves work.
- Learning networks are communities of practice. They share knowledge, compare practice & build shared capability. Learning networks often excel at spread & improvement of existing practice, but only sometimes move into structured innovation work.
- Innovating (or transforming) networks are communities that combine their assets - ideas, relationships, data, capabilities - to create new value that none could produce alone. They manage collaboration as a process of experimentation: agreeing a shared outcome, running multiple connected tests of change, learning by doing & amplifying what works across the network.
https://t.co/70NcTsBLjl
Every learning network has the potential to become an innovating/transforming network. Some actions to enable this:
1. Build a foundation of strong, trusting relationships within the network, understanding each member’s starting point & motivation for change
2. Focus on helping each other to succeed; listen to each others’ stories & plans, co-coach, give advice to each other & build shared inquiry
3. Move from “sharing” or “raising awareness” to some concrete outcomes the network want to change together through collective experimentation
4. Agree some simple norms for the network so that members help each other to make progress, make it safe to try things, fail fast & share incomplete work
5. Encourage multiple, parallel tests of change around similar outcome so projects can “steal with pride” from one another & quickly refine promising ideas
6. Put simple routines in place for noticing patterns (what is shifting where & why), capturing these insights & amplifying them across the network
7. Add additional success metrics including innovations tested, adapted & adopted in multiple places
Graphic by Ed Morrison.
Content with added inspiration from @juneholley.
Want to find out more about qualitative interviewing❓
The Open University is offering a free 3-hour course 🎉
Take a look here 👇
https://t.co/KlYt6NoaTS
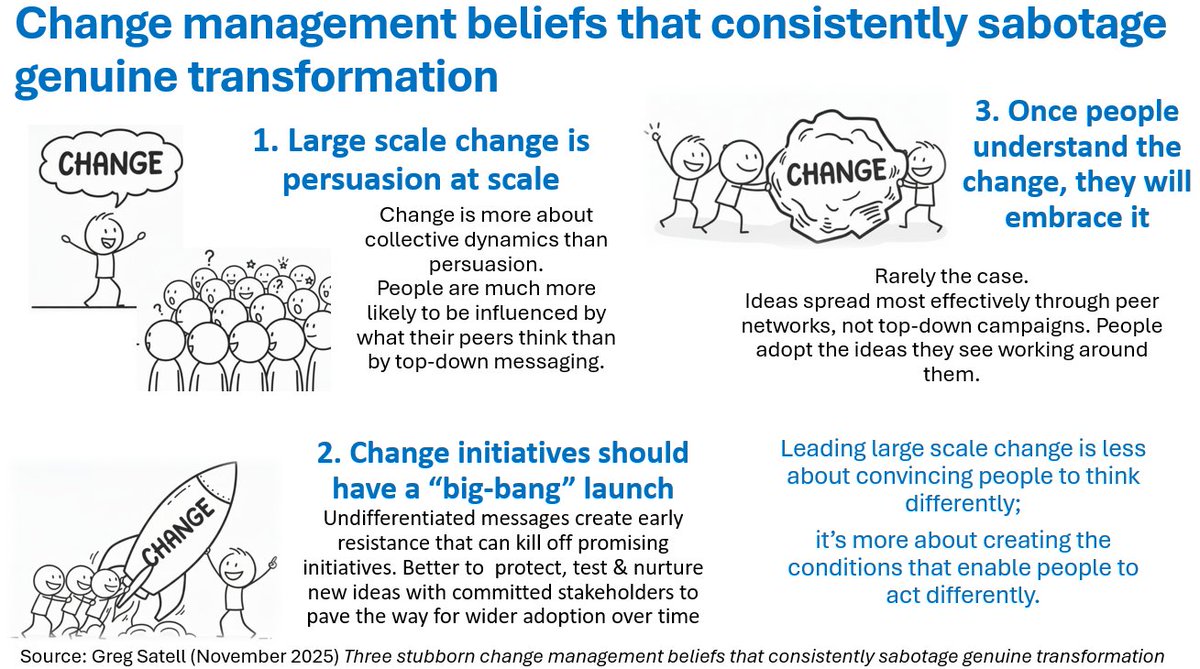
Our beliefs & assumptions about change are often the biggest barrier to leading & enabling effective change.
@DigitalTonto describes “change management beliefs that consistently sabotage genuine transformation”.
The first such belief is that large scale change is persuasion at scale; the idea that we can change opinion across an organisation by communicating a compelling case. However, change is much more about collective dynamics than about persuasion. People are more likely to be influenced by what their peers think than by top-down messaging. If we want change to spread, we need to help activate peer networks.
The second belief is that a large scale change initiative should have a “big bang” launch. The aim is to create widespread awareness that the change is happening & drive the message home. The problem is that undifferentiated messages create early resistance that can kill off promising initiatives. Much better to protect, test & nurture new ideas with committed stakeholders to pave the way for wider adoption over time, rather than trying to convince everyone at once.
The third belief is that once people understand the change, they will embrace it. The issue is that people are typically navigating many competing influences—prior beliefs, habits, social pressures & noise from many directions. That’s why ideas spread most effectively through peer networks, not top-down campaigns. People adopt the ideas they see working around them.
What might work better?
1. Deliberately starting where there’s already energy & enthusiasm & building out from a local majority (eg., three allies in a room of five) instead of trying to convert everyone first
2. Intentionally working through & connecting peer networks so people are influencing “others like us”, rather than relying on one-to-many broadcasts
3. Creating early proof through local majorities that “people like us are already doing this,” tapping into social proof rather than abstract persuasion techniques.
4. Expecting that some people will resist change & take steps to work with it, rather than assuming that better messaging will win “resistors” over
5. Focusing less on increasing information and more on enabling people to see others like them succeeding with the new behaviours, so they can appropriate and adapt the change as their own.
Leading large scale change is less about convincing people to think differently; it’s more about creating the conditions that enable people to act differently.
https://t.co/EWYFYVfxcO
during that forty five minutes, whilst you're getting ready to face the day, a man will end his days… dead from prostate cancer. Yes, one man dies every 45 minutes.
https://t.co/M7zsDDJGmJ
@smizz A book would be wonderful recording each day would be great its your journey especially as you have recorded your changing thoughts and realisations - with your beautiful images magic and inspirational