📢 🫀UK Cardiology registrars — the 2026 BJCA Training Survey is LIVE!
Have your say on cardiology training, GIM + recognise training excellence by nominating for trainer/centre of the year.
Your feedback drives change+improves training!
Find the link in the newswire or DM us
Our new textbook (Essential ECG) targeted at medical students, resident doctors and allied healthcare professionals is scheduled for release in March 2026. Pre-order your copy now! 🫀 ⚡️
https://t.co/rSTTDIFPFy
@DrDavidWarriner@DrAkshayGaur@scionpub#EPeeps#CardioTwitter
Next up: Craig Russell (arrhythmia nurse specialist) from Leeds talking about ICDs, consent and the not insignificant psychological burden.
#EPeeps#CardioEd#Cardiology@LTHTCRMandEP
🚨 Deadline extension: abstract submissions 🚨
Submitting an abstract for #BCS2026 guarantees great visibility for your work and the opportunity to interact with an engaged audience.
We've now extended the deadline to Sunday 8 February, so there's more time to get your submission in!
You can submit:
- Abstracts in basic science and clinical categories
- Case reports
- Applications for our Early Career Investigator and Michael Davies Awards
Find our more > https://t.co/TtRoOzddtr
Call for new Commissioning Editors! - 💼
Heart has a vacancy for one or more enthusiastic Commissioning Editors to help shape its scholarly agenda and contribute to strategic content development.
Commissioning Editors will be responsible for identifying topics of interest, suggesting contributors, and commissioning high-quality content across the journal’s formats. They will contribute to reviewing the submissions and participate in the journal’s editorial processes.
Further information on the role and how to apply can be found at the link below. The deadline for applications is 18th January 2026.
https://t.co/Lbt6vFDfpo
Answer to the Christmas Quiz from yesterday:
Answer:
Pulse tapping artefact
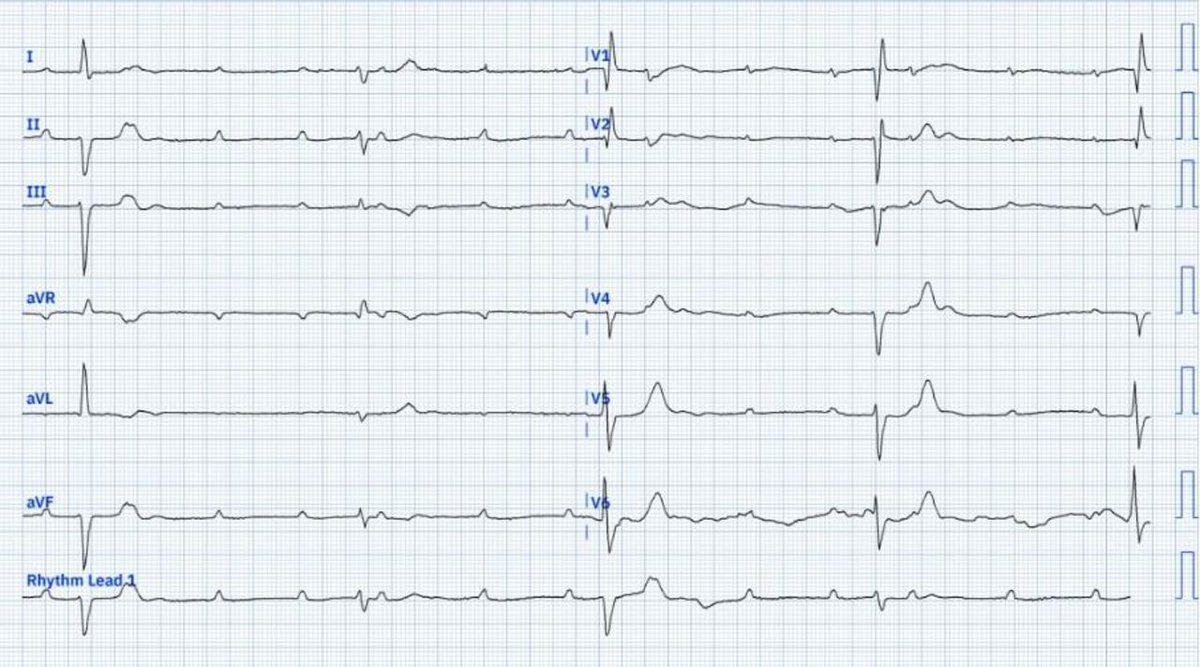
The ECG shows CHB at 25 beats per minute with ST-segment elevation in the anterior (V1–V5) and inferior (II, III, aVF) leads. Despite appearing as STEMI, several features argue against this (option A):
Horizontal ST-segment elevation is atypical for myocardial infarction.
The ST elevation does not align with a specific coronary artery territory.
Discordant ST changes are seen in V5/V6 and I/aVL.
The patient lacked a history of angina.
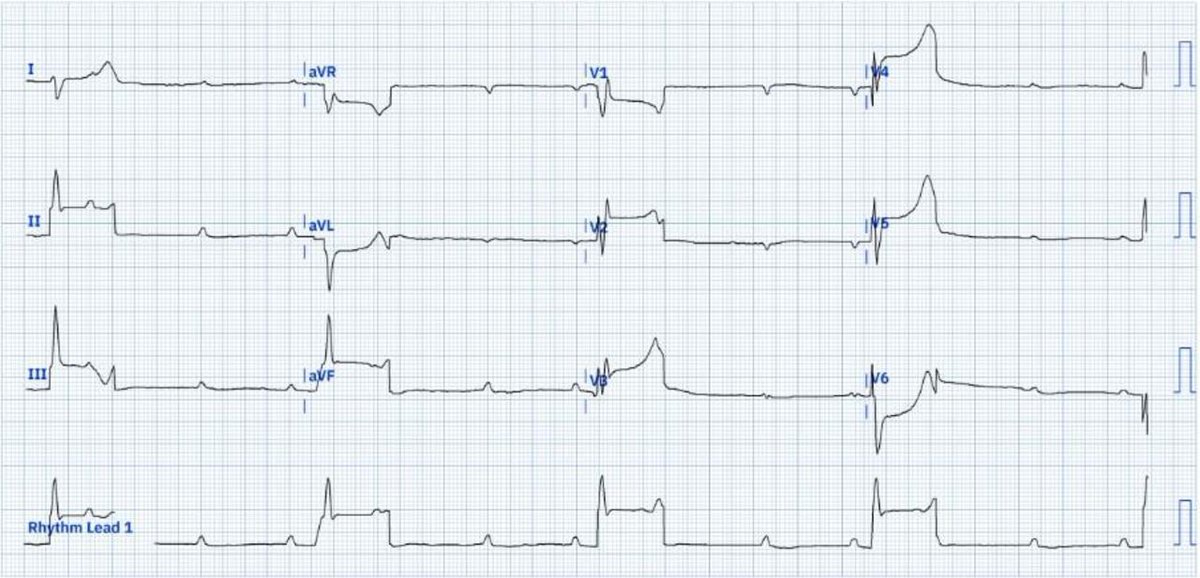
Normalisation of ST changes on a repeat ECG (see below) and normal cardiac biomarkers support an artifactual origin.
ECG artefacts can originate from cardiovascular or extracardiovascular sources. In this case, the ST-segment elevations consistently occurred after the QRS complexes, coinciding with mechanical systole. This suggests a cardiovascular source. Pulse-tapping artefacts occur when an electrode placed over an artery detects arterial pulsations, resulting in apparent ST-segment elevations. In this patient, the artefact was due to the pulsations of the left posterior tibial artery, as confirmed by unaffected leads like Lead I. Artefacts in chest leads can be explained by involvement of Wilson central terminal. (Option C)
Lead misplacement usually affects limb lead axis or causes global distortion, but here the QRS morphology is consistent and the repeat ECG is normalised without repositioning. (Option B)
Electrolytes were normal, so hyperkalaemia can be ruled out. (Option D)
The patient had a coronary angiogram, which was normal, and underwent dual-chamber pacemaker implantation.
https://t.co/5O6HU8HPnh
Christmas Quiz:
Question
What is the most likely cause of the ST-segment elevation?
Acute ST-segment elevation myocardial infarction (STEMI)
Lead misplacement
Pulse tapping artefact
Hyperkalaemia
https://t.co/LV0Px3QubD
Answer tomorrow!
I’m not entirely sure I understand how this ‘match’ works, but learning that the positions in interventional cardiology haven’t all been filled doesn’t really surprise me. Is there a vocational crisis in interventional cardiology in your area? I don’t have hard data, but my sense is that there is a shortage, and the reasons could be many: from advances in preventive therapies to professional risk, or simply lower appeal compared to other cardiovascular specialties perceived to offer more free time, less legal responsibility, and higher income for fewer sacrifices.
Excited to announce the new Geri Cards Fellowship at @UTMBHealth! 🩺❤️🧓
A 4-year integrated program (PGY4-7) offers:✅ Dual board eligibility✅Level II Imaging proficiency ✅ Research
Start: July 2026. For more info and application: https://t.co/jigbl8hzEa