Halloween Haunt: Male 60s with chest pain for 1 hour, EKG with STE in AVR & wide spread depressions. Hemodynamically stable ➡️ CCL ➡️ here’s what angio showed. After the second Left cors shot became acutely 🤢, hemodynamics collapsed hypotension + respiratory failure.
What would you do next?
Great result and display of escalation of technique to optimize the result. Were you happy with the end result of Lm-LAD? Infrequently, there is no answer to these nodules despite the utilization of all the tools. Lucky for you the LM-LCx is already stented so you could use a DCB there! Great that we are no longer living in a time compelled to put another layer of stent in that LCx.
10/ My last and most important message
It isn't just your hard work that built your interventional career- it's also the sacrifice, blood and sweat of those who love you
Gene Braunwald died at 96.
In a normal world, this would be front page of the NYT and WSJ.
The father of modern cardiology.
Fled the Holocaust as a boy
Went on to save millions of lives
The most important clinician-scholar of the last 50 years. We should all know his name
Nice demonstration! Many nuances to this, back in the day were leaving the sheath it but have not done so for a few years now. Angle of entry (more parallel to the skin), anterior puncture, less movement/trauma during peel away, placing 3-4 gauze to keep angle 120-140 degrees all helpful. Sometimes, they just bleed! Subcu epi/lido injection, bone wax, pressure dressings, and mattress sutures all helpful.
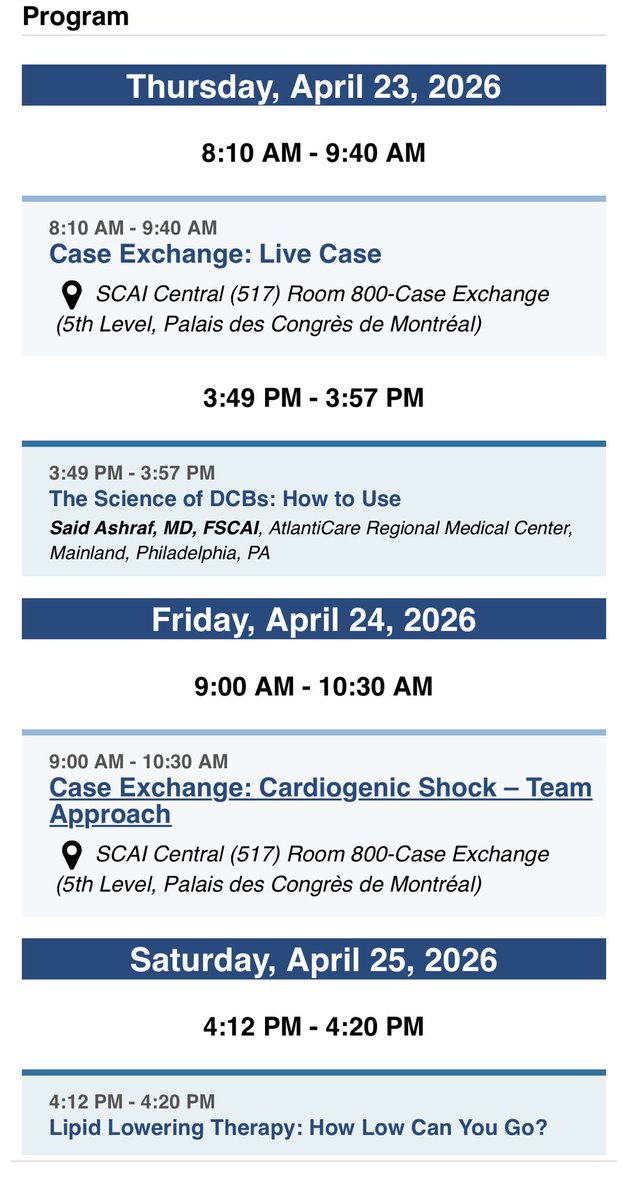
Excited to attend #SCAI2026 in Montréal this week! Looking forward to a week of cutting-edge science.
I’ll be presenting on Drug-Coated Balloons (DCB) & Lipid Lowering Therapy, paneling Cardiogenic Shock Team case exchange and a live case from Oman! — come join the conversations! 🎈💉
Registration is still open—don't miss out on the best in #InterventionalCardiology. See you there!
Are you ready?! Stenty can’t wait to welcome you to #SCAI2026 next week—bringing you cutting-edge science, live cases, and the latest innovations in #InterventionalCardiology. Have you built your schedule?
Explore the program ➡️ https://t.co/Cp2jslPYHo
Register ➡️ https://t.co/z5iwU1PtJP
#AdventuresOfStenty #CardioX #SCAIHatDay
I learned from @homam_heartdoc to create a small incision with scalpel after removing the micro puncture sheath and pushing a hemostat down to the arteriotomy site overriding the 0.035” J wire, so as to create a clear track & get subcu tissue out of the way. Much smoother deployment, can’t recall last time I had any problems with Perclose and I use it a lot.
In any case! I don’t think this will be a durable result. My understanding & experience with these types of resistant nodules has taught me that they continue growing & despite aggressive modification they return to haunt. had a case where it protruded right through the stent strut exactly 1 year later. Time will tell with this one. Curious to hear your Thoughts?
@realarainmd CP, +EKG changes, +DAPT loaded, prox LAD with large area of myocardium in jeopardy. Hemodynamics stable. Didnt know Lvef at the time of decision making. +experience in dealing with these helps
Have been in these scenarios before. EKG with stemi and active chest pain, a couple of angios showing transient recanalization, stop and bring back later or send to CTS, only for vessel to close again & come back to the lab after cardiac arrest in shock. With active chest pain and EKG shows STEMI with large area of myocardium at risk loaded with DAPT - pci first.
@EdmondOwen8 Perhaps. I think in modern era the rate of stemis going for cabg are <2%. Did have a discussion with the surgeon midway through the case, had OA not modified the plaque ,
Wouldve probably sent to surgery; patient was loaded with aspirin and ticagrelor before the procedure started