💪El músculo es mucho más que movimiento: es un órgano endocrino.
Revisión reciente destaca que las mioquinas liberadas durante el ejercicio regulan metabolismo, inflamación, insulina, tejido adiposo y envejecimiento saludable.
HER2+ THERAPY IS BECOMING RESPONSE-ADAPTED
A simple algorithm proposed by Tarantino et al. (JCO 2026):
▪️ Stage IIA → THP → Surgery → HP
▪️ Stage IIB → THP → Response assessment → Continue THP or escalate to T-DXd
▪️ Stage III → TCHP or THP → T-DXd → Surgery
▪️ pCR → Complete planned HER2-directed therapy
▪️ Residual disease → T-DXd or T-DM1
The concept is simple:
✓ Stage
✓ Biology
✓ Treatment response
Together determine treatment intensity.
We are moving beyond a one-size-fits-all approach toward more personalized HER2-directed therapy.
Adapted from Tarantino et al., JCO 2026.
#BreastCancer #HER2 #HER2Positive #Oncology #JCO #ASCO #TDXd
One of the most important data points from the OPTIMA trial presented at #ASCO26, in my view, is this: 67.8% of patients with ER+/HER2− early breast cancer who were considered clinically high risk were found to be genomically low risk and did not receive chemotherapy.
This population represents a group of patients who, in daily practice, would often be offered chemotherapy. Nodal involvement, larger tumor size, grade, and other clinicopathologic risk factors traditionally push us toward labeling these patients as “high risk.” Importantly, the study was not limited to patients with 1–3 positive nodes; patients with 4–9 positive nodes, including N2-level disease, were also included.
That is why the message of OPTIMA matters: clinical risk and genomic risk are not the same thing. In luminal breast cancer, tumor burden may be high, but that does not necessarily mean the tumor biology is likely to derive meaningful benefit from chemotherapy.
In the genomically low-risk group, the contribution of chemotherapy appears to be absent or, at best, very limited. When the absolute benefit is this small, the acute and long-term toxicity burden of chemotherapy can easily offset that potential gain.
When interpreting the results in premenopausal patients, it is important to remember that endocrine therapy was given with OFS. This is relevant to the discussion that part of the chemotherapy benefit seen in younger patients may be related to ovarian suppression. However, the exclusion of patients younger than 40 years is also a clear limitation; these data should not be directly extended to very young patients. (Of course, these limitations should be acknowledged: the follow-up is still relatively short, some key subgroups remain small, and the results should be applied within the population studied.)
The cost-effectiveness analysis has not yet been reported. However, if approximately two-thirds of clinically high-risk patients can safely avoid chemotherapy, the potential health-economic value of this approach is obvious.
This should no longer depend solely on individual physician preference or a patient’s ability to pay. Genomic assays such as Prosigna, Oncotype DX, and MammaPrint should become a standard part of reimbursement policy within their validated indications and appropriate eligibility criteria.
We are now in the second quarter of the 21st century. In ER+/HER2− early breast cancer, making treatment decisions based only on tumor size and nodal status is no longer sufficient. We should be able to offer biology-driven treatment decisions to patients in a fair and accessible way.
Estradiol 0.01% cream.
Sig: apply 1 gram nightly for 2 weeks, then 1 gram twice a week forever.
For all your menopausal patients. Every damn one. The rate of UTIs will plumet around the world.
Make your smart phrases.
Dispense liberally.
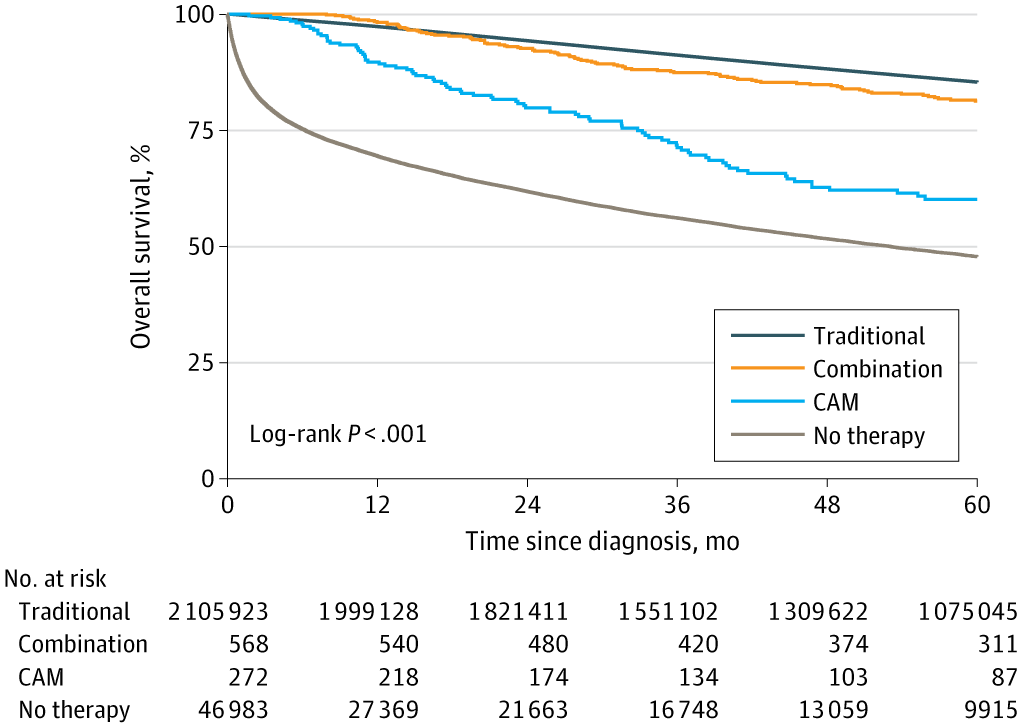
For breast cancer, alternative medicine alone was linked to a 267% higher mortality hazard.
Even when combined with standard treatment, mortality hazard was still 45% higher.
Modern oncology saves lives. Please consider using it.
🌸An ongoing phase III trial addressing unmet clinical needs
🌸Abemaciclib for locoregional recurrence of HR+HER2- breast cancer (JCOG2313, AURA trial, NCT07190443) #JCOG#JCOG2313#AURA
https://t.co/TFeuWdfkIS