🌀 7 CAUSES OF VERTIGO
Vertigo is a symptom, not a diagnosis.
When a patient complains of “dizziness,” the key question is:
❓ Is this true vertigo (a false sensation of movement) or something else?
Correctly distinguishing peripheral from central causes is essential, as some causes are benign, while others may represent a neurological emergency.
🔑 Common Causes of Vertigo
1️⃣ BPPV (Benign Paroxysmal Positional Vertigo)
• Most common cause
• Brief episodes triggered by head movement
• No hearing loss
• Positive Dix-Hallpike test
• Treated with the Epley manoeuvre
2️⃣ Vestibular Neuritis
• Acute severe vertigo lasting days
• Often follows a viral illness
• Nausea and vomiting common
• No hearing loss
3️⃣ Ménière Disease
• Recurrent episodes of vertigo
• Fluctuating hearing loss
• Tinnitus and aural fullness
• Usually unilateral
4️⃣ Vestibular Migraine
• Vertigo associated with migraine features
• Photophobia, phonophobia, aura
• May occur without headache
5️⃣ Labyrinthitis
• Vertigo + hearing loss
• Often post-viral
• Auditory and vestibular symptoms occur together
6️⃣ Acoustic Neuroma (Vestibular Schwannoma)
• Progressive unilateral hearing loss
• Tinnitus
• Gradual onset imbalance or vertigo
7️⃣ Central Causes 🚨
• Stroke
• Multiple sclerosis
• Cerebellar tumours
• Brainstem lesions
⚠️ Red Flags Suggesting a Central Cause
🚨 Diplopia
🚨 Dysarthria
🚨 Limb weakness
🚨 Severe ataxia
🚨 New headache
🚨 Persistent neurological deficits
🩺 Clinical Approach
✔️ Take a careful history
✔️ Examine for nystagmus
✔️ Perform the HINTS examination when appropriate
✔️ Assess hearing
✔️ Look for focal neurological signs
💡 High-Yield Pearl
Peripheral vertigo is common, but never miss a central cause.
Remember:
🧠 Acute vertigo + neurological signs = Stroke until proven otherwise.
📚 Save this post and visit our website for innovative high-yield medical notes:
https://t.co/Ivljom1DDe
#Vertigo #Neurology #BPPV #MeniereDisease #vestibularneuritis
14 Features to Analyze on Every ECG
1. Standardization (calibration) and technical quality
2. Heart rate(s): atrial and ventricular if not the same
3. Rhythm/AV conduction
4. PR (AV) interval
5. QRS interval (width)
6. QT/QTc intervals
7. QRS axis
8. P waves (width, amplitude, shape)
9. QRS voltages: normal, high or low
10. R wave progression in chest leads
11. Q waves (normal vs. abnormal)
12. ST segments
13. T waves
14. U waves
Potassium disorders can become life-threatening long before symptoms appear.
For every nurse, ECG interpretation is just as important as checking the potassium level.
Remember: ⬆️ Hyperkalemia → Peaked T waves, widened QRS, risk of cardiac arrest. ⬇️ Hypokalemia → Flat T waves, prominent U waves, ventricular arrhythmias.
Always monitor the ECG, identify the underlying cause, and correct potassium abnormalities safely.
A simple electrolyte imbalance can quickly become a cardiac emergency.
#NinjaNursing #Potassium #ECG #SNLE
https://t.co/knvd83SjlI
هل يمكن أن تكون عندك مشكلة في الكلى مع ان وظائف الكلى مثل الكرياتينين طبيعية🤔؟
نعم ممكن
عشان كذا الطبيب لا يعتمد فقط على تحليل الكرياتينين بل قد يطلب أيضا فحص زلال البول (UACR)
لأنه يساعد على اكتشاف أي ضرر في الكلى في وقت مبكر خصوصاً للمصابين بالسكري
طيب ممكن تشرح إذا ماعندي أي أعراض
ليه أسوي الفحص؟
السبب أن اكتشاف الزلال في وقت مبكر يساعد على بدء العلاج بأدوية تقلل الزلال وتبطئ تدهور وظائف الكلى وتقلل من خطر الوصول إلى الفشل الكلوي
💡 هل طبيعي تكون كليتك تعبانة.. وفحص الكرياتينين سليم؟
نعم، وبشدة وهذا هو السر الذي يجعل الأطباء لا يعتمدون على الكرياتينين وحده، بل يطلبون فحص زلال البول (ACR / UACR) كإنذار مبكر يكشف الضرر الصامت قبل أن يظهر في الدم.
🛑 لكن أنا ما عندي أي أعراض، ليه أسوي الفحص؟
هنا تكمن الخدعة.. الكلى تتأذى بصمت واكتشاف الزلال مبكراً يحميك قبل أن تشتكي عبر أدوية تبطئ تدهور الكلى وتمنع الوصول للفشل الكلوي.
🔬 كيف تقرأ النتيجة مخبرياً؟
[ألبومين mg ÷ كرياتينين g]
🟢 طبيعي: أقل من 30 mg/g
🟡 ارتفاع بسيط (خطر صامت): 30 – 300 mg/g
🔴 ارتفاع كبير (تلف واضح): أكثر من 300 mg/g
⚠️ تنبيه للمريض والمخبري: الجفاف أو المجهود البدني العنيف قبل الفحص يعطي نتيجة إيجابية كاذبة، لذا يجب تجنبهما أو إعادة الفحص للتأكد.
DKA is one of the few endocrine emergencies where the order of treatment matters as much as the treatment itself ⚠️🩺
📌 Confirm the diagnosis
📌 Start IV fluids immediately
📌 Check potassium before insulin
📌 Begin insulin infusion when appropriate
📌 Monitor the anion gap until it closes
Remember:
💧 Fluids first.
⚡ Potassium always.
💉 Insulin after potassium is safe.
Never stop the insulin infusion until ketoacidosis has resolved—even if the blood glucose has normalized.
A practical review of diabetic ketoacidosis covering diagnosis, ABG interpretation, fluid resuscitation, insulin therapy, potassium replacement, and high-yield emergency medicine pearls 📚🩺
https://t.co/1dSdJ0pv1C
Influenza vaccination in adults: annual, age-appropriate protection before each flu season
Flu vaccination is not only for older adults. The current approach is annual vaccination for everyone ≥6 months, with enhanced vaccine options preferred in adults ≥65 years when available
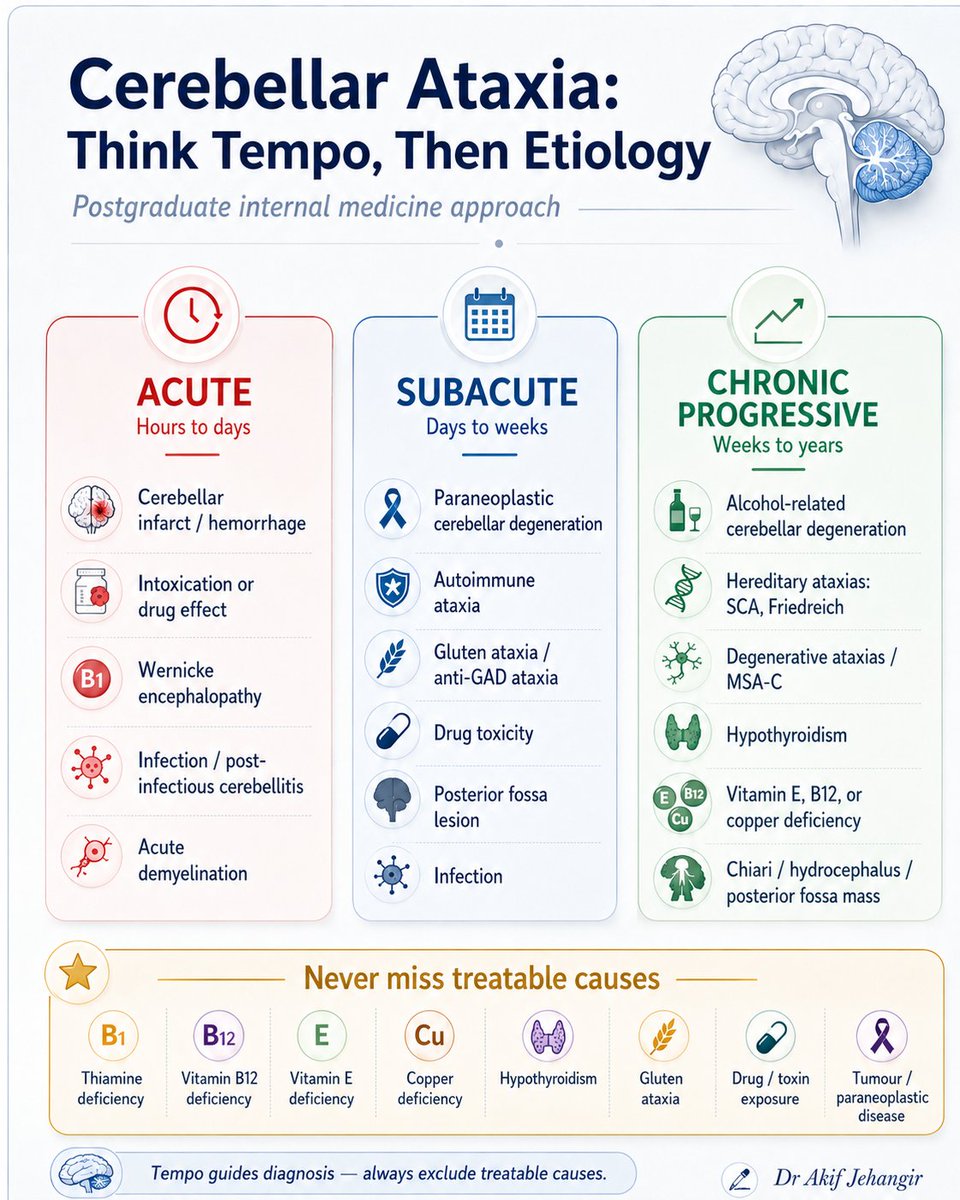
Cerebellar ataxia should be approached by tempo of onset rather than by memorising isolated causes.
First decide whether the presentation is acute, subacute, or chronic progressive, then narrow the differential and actively look for treatable causes before calling it degenerative
Adult-Onset Still’s Disease: Recognising the Typical Rash
An evanescent salmon-pink rash with spiking fever is a classic clue to adult-onset Still’s disease. A concise high-yield review for clinicians and trainees.
#InternalMedicine
Podagra: Recognising Acute Gout at the 1st MTP Joint
A red, hot, swollen 1st MTP joint is classic for podagra. A high-yield review highlights the key clinical clues, diagnosis, acute flare treatment, urate-lowering therapy, and the important differentials you should never miss.
💊DRUG OF THE DAY #024: CIPROFLOXACIN
⚠️ EDUCATIONAL ONLY, NOT A MEDICAL ADVICE.
LICENSED PHARMACIST SHARING GENERAL DRUG INFORMATION.
CONSULT YOUR DOCTOR OR PHARMACIST BEFORE MAKING ANY CHANGES TO YOUR TREATMENT.
Ciprofloxacin is a fluoroquinolone antibiotic used to treat a wide range of bacterial infections, particularly those caused by Gram-negative organisms. It is commonly prescribed for urinary tract infections, gastrointestinal infections, certain respiratory tract infections, bone and joint infections, and some healthcare-associated infections.
Ciprofloxacin works by inhibiting bacterial DNA gyrase and topoisomerase IV, enzymes essential for bacterial DNA replication and cell division. This results in rapid bacterial death and makes ciprofloxacin a bactericidal antibiotic.
📌 Key Clinical Pearl:
Fluoroquinolones are highly effective antibiotics, but they should be reserved for situations where their benefits outweigh potential risks. Appropriate use helps reduce antimicrobial resistance and prevent avoidable adverse effects.
✅ Broad Gram-negative bacterial coverage
✅ Excellent oral bioavailability
✅ Available in oral and intravenous formulations
✅ Useful in complicated urinary tract infections
✅ Effective against several serious bacterial infections
⚠️ Tendinitis and tendon rupture may occur
⚠️ QT interval prolongation is possible
⚠️ May cause central nervous system effects (dizziness, confusion)
⚠️ Overuse contributes to antimicrobial resistance
As pharmacists, we play an important role in antimicrobial stewardship by ensuring appropriate antibiotic selection, reviewing drug interactions, counseling patients on administration, and promoting responsible antibiotic use.
"The most effective antibiotic is the right antibiotic not necessarily the broadest one."
#DrugOfTheDay #Ciprofloxacin #Fluoroquinolone #Antibiotics #AntimicrobialStewardship #ClinicalPharmacy #DrugSafety #InfectiousDiseases #HospitalPharmacy #PharmaAmeer
https://t.co/OrFh2s6CBQ
Brugada ECG: Type 1 = diagnostic coved ST↑ (≥2mm) in V1-V3 with inverted T. Types 2/3 show saddleback patterns (non-diagnostic) — sodium blocker challenge may unmask Type 1. 🫀⚡️
#BrugadaSyndrome#Cardiology#ECG#Arrhythmia#SuddenCardiacDeath









































![AliAl_khalifah's tweet photo. 💡 هل طبيعي تكون كليتك تعبانة.. وفحص الكرياتينين سليم؟
نعم، وبشدة وهذا هو السر الذي يجعل الأطباء لا يعتمدون على الكرياتينين وحده، بل يطلبون فحص زلال البول (ACR / UACR) كإنذار مبكر يكشف الضرر الصامت قبل أن يظهر في الدم.
🛑 لكن أنا ما عندي أي أعراض، ليه أسوي الفحص؟
هنا تكمن الخدعة.. الكلى تتأذى بصمت واكتشاف الزلال مبكراً يحميك قبل أن تشتكي عبر أدوية تبطئ تدهور الكلى وتمنع الوصول للفشل الكلوي.
🔬 كيف تقرأ النتيجة مخبرياً؟
[ألبومين mg ÷ كرياتينين g]
🟢 طبيعي: أقل من 30 mg/g
🟡 ارتفاع بسيط (خطر صامت): 30 – 300 mg/g
🔴 ارتفاع كبير (تلف واضح): أكثر من 300 mg/g
⚠️ تنبيه للمريض والمخبري: الجفاف أو المجهود البدني العنيف قبل الفحص يعطي نتيجة إيجابية كاذبة، لذا يجب تجنبهما أو إعادة الفحص للتأكد.](https://pbs.twimg.com/media/HL7bGlHboAAJ4id.jpg)