لأول مرة في المملكة، نجح #التخصصي في علاج عدد من المرضى الذين يعانون من انسداد وتضيق الشرايين الطرفية تحت الركبة، باستخدام تقنية مبتكرة تعتمد على إدخال دعامة حديثة تلقائية التحلل عبر قسطرة دقيقة في الفخذ، دون الحاجة إلى جراحة مفتوحة مما أسهم في استعادة تدفق الدم، وتخفيف الألم، وتسريع التئام الجروح، والحد من خطر البتر.
لمزيد من المعلومات: https://t.co/KAO4DVl8mc
فالذنب لا يخلو من عقوبة البتة، ولكن لجهل العبد لا يشعر بما هو فيه من العقوبة؛ لأنّه بمنزلة السكران والمخدَّر والنائم الذي لا يشعر بالألم، فإذا استيقظ وصحا أحسّ بالمؤلم.
فترتّبُ العقوبات على الذنوب كترتب الإحراق على النار، والكسر على الانكسار ، والإغراق على الماء، وفساد البدن على السموم.
وقد تقارن المضرة للذنب، وقد تتأخر عنه إمّا يسيرًا وإمّا مدةً.
وكثيرًا ما يقع الغلط للعبد في هذا المقام، ويذنب الذنب فلا يرى أثره عقيبه، ولا يدري أنه يعمل عمله على التدريج شيئًا فشيئًا .. فإنْ تدارك العبدُ بالأدوية والاستفراغ والحمية وإلا فهو صائر إلى الهلاك.
#ابن_القيم "الداء والدواء" (٢٧٢)
2/2
Claim: Treatment “might” not follow “standard of care”
Response: This is the real reason why those opposing physicians bring this issue. Fear of losing patients is perceived is a threat. Why would anyone with a competing treatment try to prevent patients from getting it? If your proposed treatment is better, you should not be concerned. If its inferior, you are liable ethically and medically if you still promote your treatment. If you are not sure, educate yourself before reaching conclusions. Standard of care is not based on or determined by a speciality or a society. Science and data determine this. Some society guidelines contradict other societies’ own guidelines. Obesity guidelines (Bariatric, endocrine, endoscopists, family) is a good example. No one owns a patient. No one owns a disease.
As we said before, medicine evolves. IR has become a clinical service in many countries. For example, the USA with the new IR board certification (which I hold), direct residency, inpatient service, and probable need for subspecialties with the expanding treatments would only serve to provide better, more efficient, and cost effective patient care. This is happening and will be the norm soon.
Claim: IR cannot accept ER admission.
Response:This is simply wrong. Some places with large enough IR service/support are already doing this. Do we admit all patients? No. A healthy child with fracture can be admitted under orthopedic surgery while a child with DM, poor nutrition and fractures from NAT will be admitted under peds. A patient with post sleeve leak will be admitted under surgery while a patient with post sleeve PE will be admitted under medicine. A patient with post IR procedure pain can be admitted under IR for pain control while a patient with dislodgment of a recent fresh g tube will be admitted under surgery.
If you believe in providing best care for patients, you shouldn’t feel threatened. The clinical IR practice is happening in many places. Whats holding this from happening in the rest, is simply the lack of manpower. In few years, independent clinical IR will be universal.
1/2 We have been noticing a trend from some physicians from other specialties, whom IR offer competing options to their treatments, to try and underestimate the IR clinical practice.
Claim: IR should not do X procedure, what if complications happen?
Response: Majority of IR practice involve treating complications of other services. Post surgical abscesses, bleeding, biliary/urinary obstructions/leaks, access sites complications, etc. If a complication happens to any physician, the consulted service HAS to respond and manage it. Whether IR were consulting or being consulted, there is no difference. This is healthcare and responding to manage complications is not an option, no one can refuse. If a complication happens and the consulted service refuses, simple documentation would put the refusing physician liable.
Claim: IR can not run clinics
Response: Clinic is a space that allows physician/patient interaction in outpatient basis. Patients need to hear from the specialist the details of the proposed treatment plan before committing to admission. Its not just for providing procedures and peri procedure care. Follow up and long term management of certain patients population. Examples of these patients that need indefinite follow up/management from the time of presentation are numerous; vascular anomalies, families with HHT, patients dependent on tubes, dialysis pts, etc. Clinics are important for most specialties. This is true for anesthesia (pre-op,..), rad onc, genetics, pain clinic, etc.
Claim: IR do not admit patients
Response: Medicine evolves. Nationally and internationally, minimally invasive procedures are most commonly done as day procedures with short stay admission. This has well known advantages over wasting hospital resources with admission, anesthesia booking, OR time. This is true for IR procedures, endoscopy, pain interventions, cosmetic, and other procedures. All of these services provide admission for their patients. In very few IR cases, full admission can be done safely for post procedure pain/nausea control. This is true for oral/OMF surgeons from dental background, pain service from anesthesia background, and now recently for radiation oncology.
الفروقات الرئيسية تكون بنسبة النجاح وامان الاجراء التي لم يتم التطرق لها.
الكثير من المغالطات المذكورة @drnaifalhathal:
١- نسبة الرجوع اقل مع القسطرة بسبب علاج الارتجاع الاساسي بالظهر (سيتم توضيح ذلك بالدراسات العلمية المنشورة من قبل جراحين مسالك بولية)
٢- القسطرة تعالج الدوالي الداخلية (بالظهر والعانة) والخارجية من الفخذ وشبكة الدوالي حول الخصية (#الأشعة_الصوتية بعد الاجراء توضح ذلك بسهولة ولا يمكن اخفاؤها)
٣- الاشعاع المستخدم اقل من اشعة الصدر العادية (اقل جرعة اشعاع من مجرد سفرك بالطائرة للرياض!)
٤- الصبغة التي تحقن لا تؤثر على الكلى لمن لا يشكو من قصور كلوي وتخرج الصبغة من الجسم خلال دقائق ونراها بالاشعة في نهاية الاجراء بالمثانة.
ماذا عن نسبة حدوث قيلة مائية مزمنة؟ التخدير؟ شق جراحي بمنطقة العانة؟ خطر اصابة شرايين الخصية وضمورها؟ ترك دوالي صغيرة لا يمكن رؤيتها بالميكروسكوب؟ كلها مخاطر جراحية لا تحدث عند العلاج بالقسطرة.
#استشر_طبيب_الأشعة_التداخلية_بنفسك
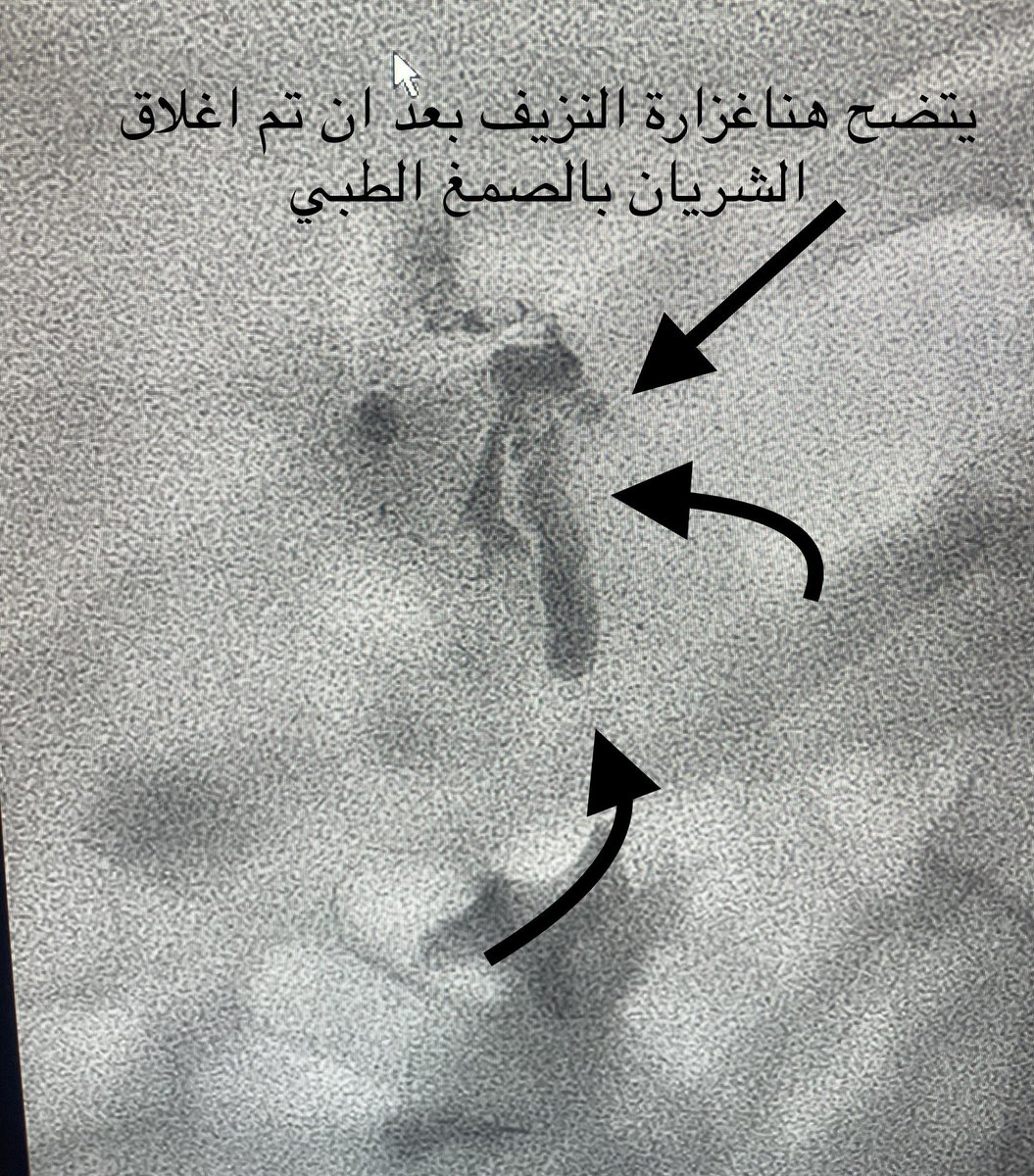
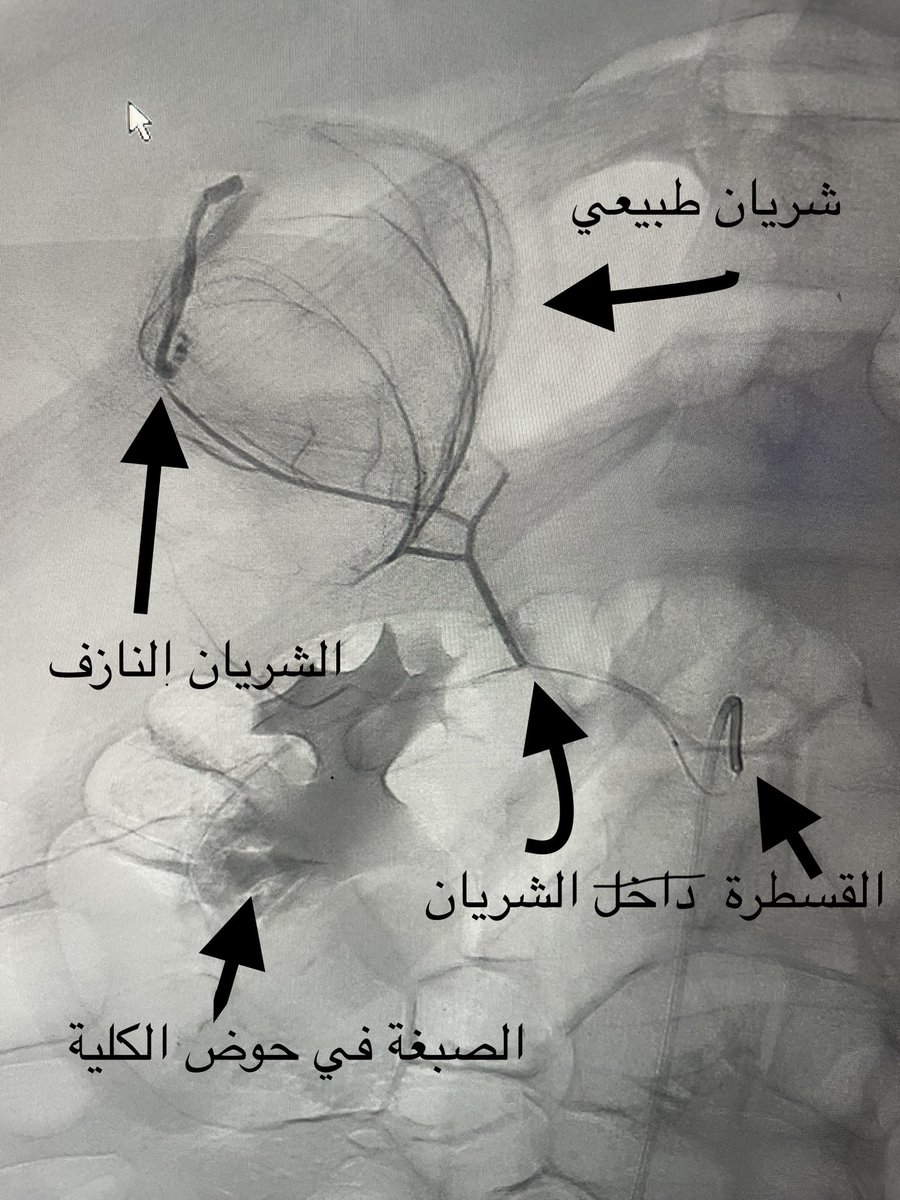
شاب لدية ، نزول حاد في الصفائح وزيادة سيولة الدم مع فشل الوسائل للتحكم في النزيف الداخلي حيث تطلب نقل مالايقل عن ٦ وحدات دم ، تم التدخل ولله الحمد وانقاذ حياة المريض وايقاف النزيف بالصمغ الطبي مع تحسن واستقرارالوظائف الحيوية 😄👍🏻
Participate in SIRS2022, the 6th Annual Scientific Meeting and Workshops of SIRS, held at Hilton, Jeddah, from 10-12 November 2022. Learn more: https://t.co/zhqtwY6wyh @sirs_ksa
Join us at our 22nd Riyadh Interventional Radiology Club on the 28th of September 2022!
-Geniculate Artery Embolization-
.
.
.
🗓 28th September 2022
🕖 20:00 - 21:45
🎓CME Accreditation
@SchsOrg#بدون_جراحة