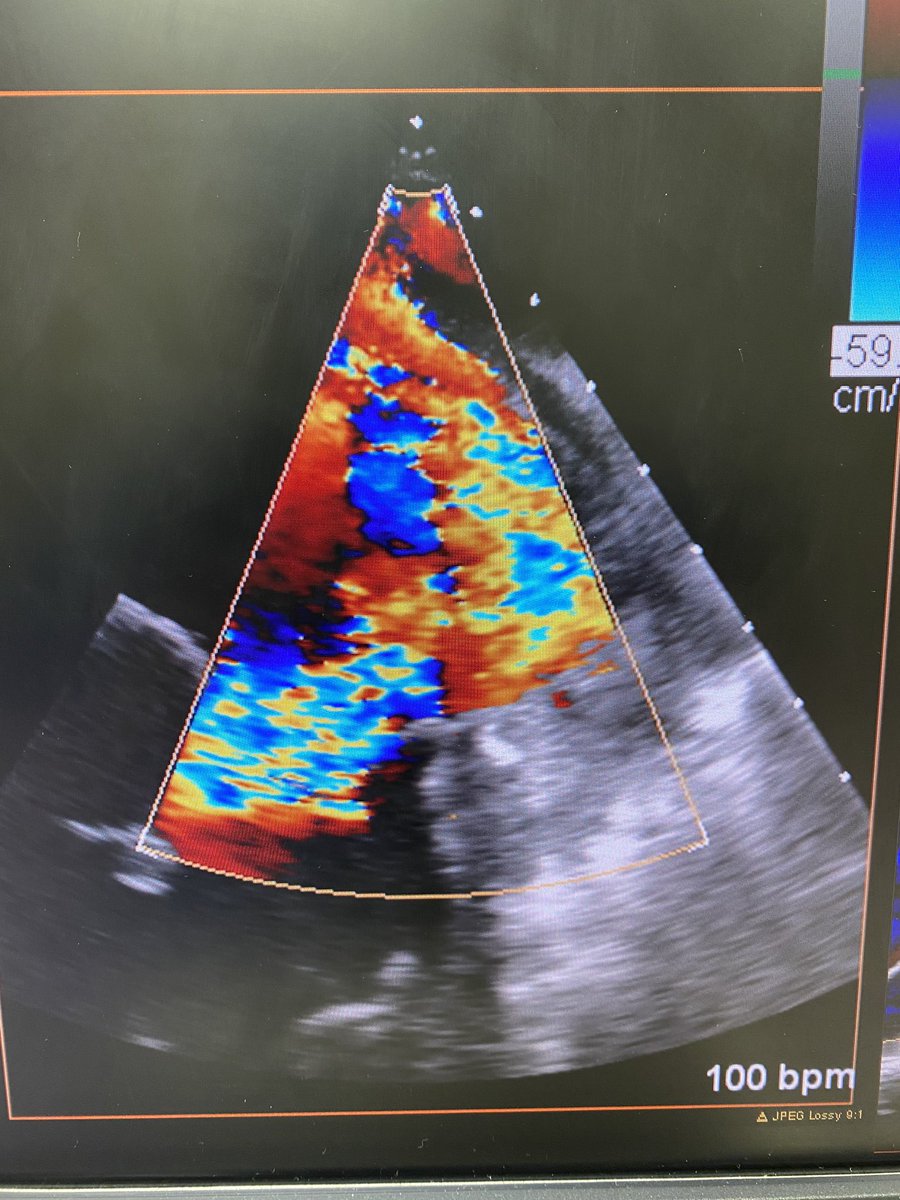
Pt sp sternotomy x2 presents w/new onset HFrEF likely 2/2 severe AI. Currently with mechanical MV and tricuspid ring. Minimal TR, normal MV function. TTE with depressed EF, severe AI, normal leaflets. CT w/no leaflet Ca2+, mechanical MV right up against NCC. What do you do?
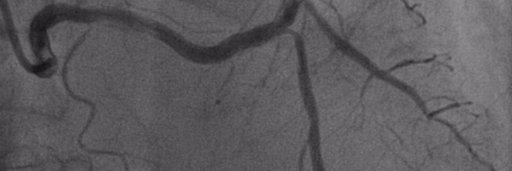
70's, DM, ESRD, CVA, frail, prior PCI to prox LAD and OM1, presents with NSTEMI. Angio shows L dominant, short LM with severe disease (abnormal dFR in LAD and LCx). Referred for CABG, turned down at 2 different centers. 2 admissions in a month for syncope/CHF. Referred for PCI
https://t.co/Dgui02GotO The most pressing issues that they identify are the increase in late presentation for STEMI and an increase in AS mortality in patients awaiting TAVR...two of the areas where we clearly know our services provide improvement in morbidity and mortality...
71yo at high surgical risk came in w/acute worsening of his known MR and cardiogenic shock. IABP placed, too sick for surgery, referred for clip. LA pressures were impressive. Bileaflet prolapse.
Interesting physiology case. 65yo woman w/very anginal sounding cp comes to my clinic. Low risk, I start beta blocker, max it out. She feels a little better, I start Ca2+ blocker, max it out. She still has angina. So I do a treadmill stress echo. Clear stress induced ant wma.