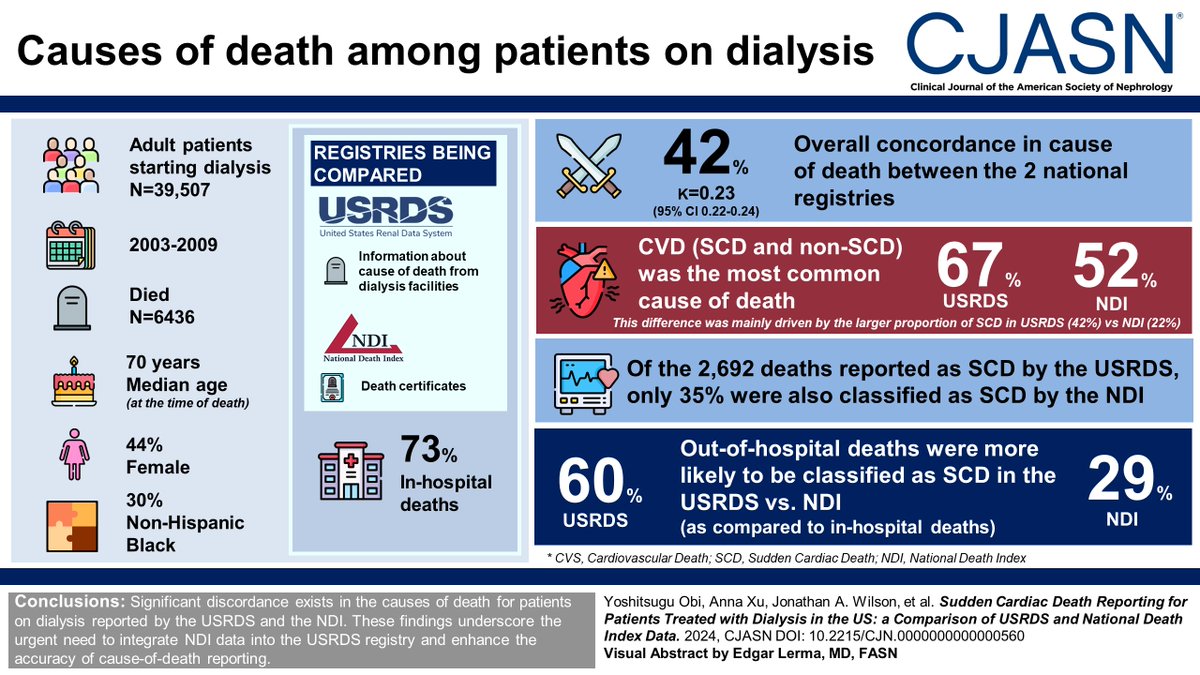
Cause-specific mortality data from the United States Renal Data System (USRDS) form the basis for identifying cardiovascular disease (CVD), specifically sudden cardiac death (SCD), as the leading cause of death for patients on dialysis. This study found that significant discordance exists in the causes of death for patients on dialysis reported by the USRDS and the NDI. https://t.co/U0EilIHWn5
@DanTheKidneyMan
@DrTariqShafi
@Yoshi_Obi
Dialysis #Symptom index burden & #SymptomClusters in a prospective cohort of dialysis patients #MADRAD
Most common symptoms:
Tired/lack of energy 71%,
Dry skin 62%
Trouble falling asleep 44%
Muscle cramps 43%
Itching 43%
https://t.co/pJhXe1jDuk
#Cramps#Pruritus@ConnieMRhee
Now open access in @NDTsocial
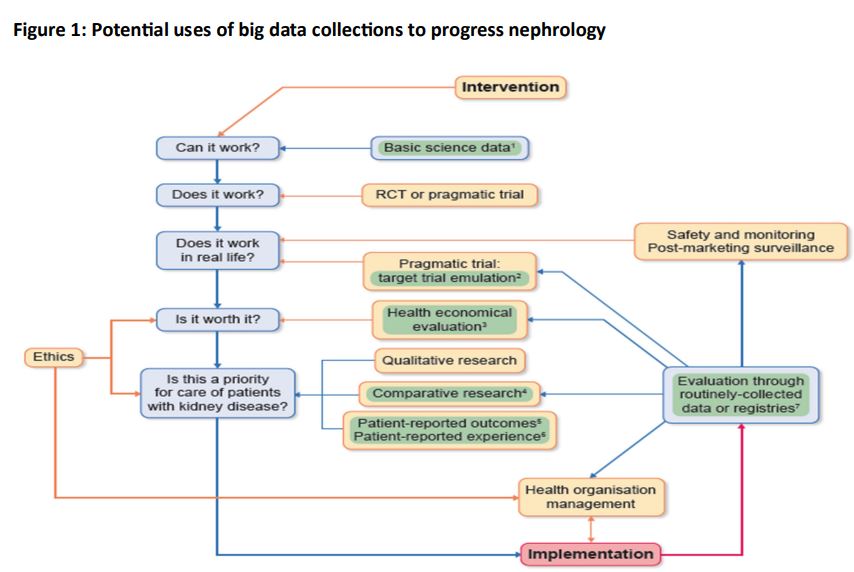
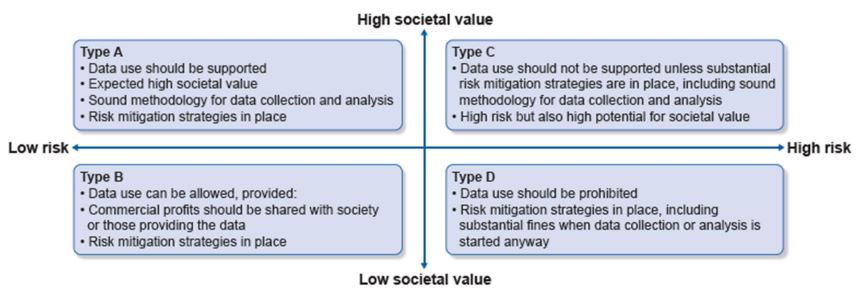
Ethical considerations on the use of big data and AI in kidney research from the ERA ethics committee
🧐Analysis observational data, prone to many biases, can finally result in low-quality medical care.
▶️https://t.co/mTTgZYVxQH
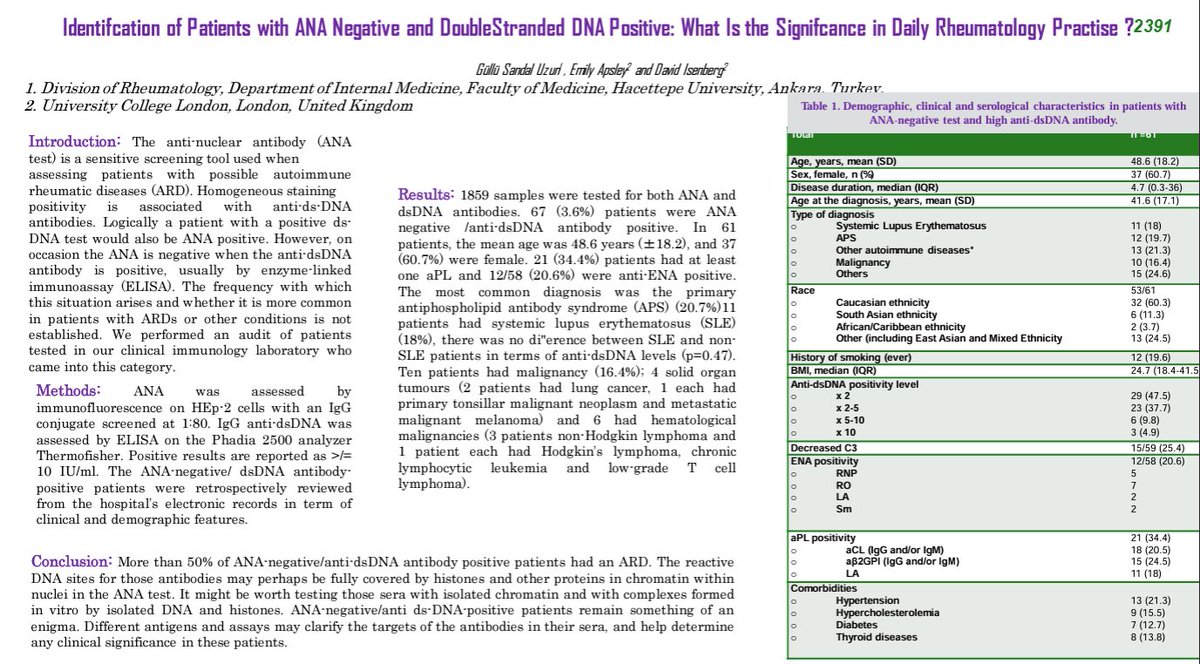
Interesting! Study of pts w/ ANA(-) & dsDNA(+). 1 in 5 dx with APLS! Have others seen that?
I have been disgregarding this pattern, though some of that is related to my in-house assay (seems overly-sensitive) & my bias against overdiagnosis
#ACR24@RheumNow Abstr#2391
Cause-specific mortality data from the USRDS form the basis for identifying CVD, specifically SCD, as the leading cause of death for patients on dialysis. This study found that significant discordance exists in the causes of death for patients on dialysis reported by the USRDS and the NDI. https://t.co/U0EilIHWn5
@DanTheKidneyMan
@DrTariqShafi
@Yoshi_Obi
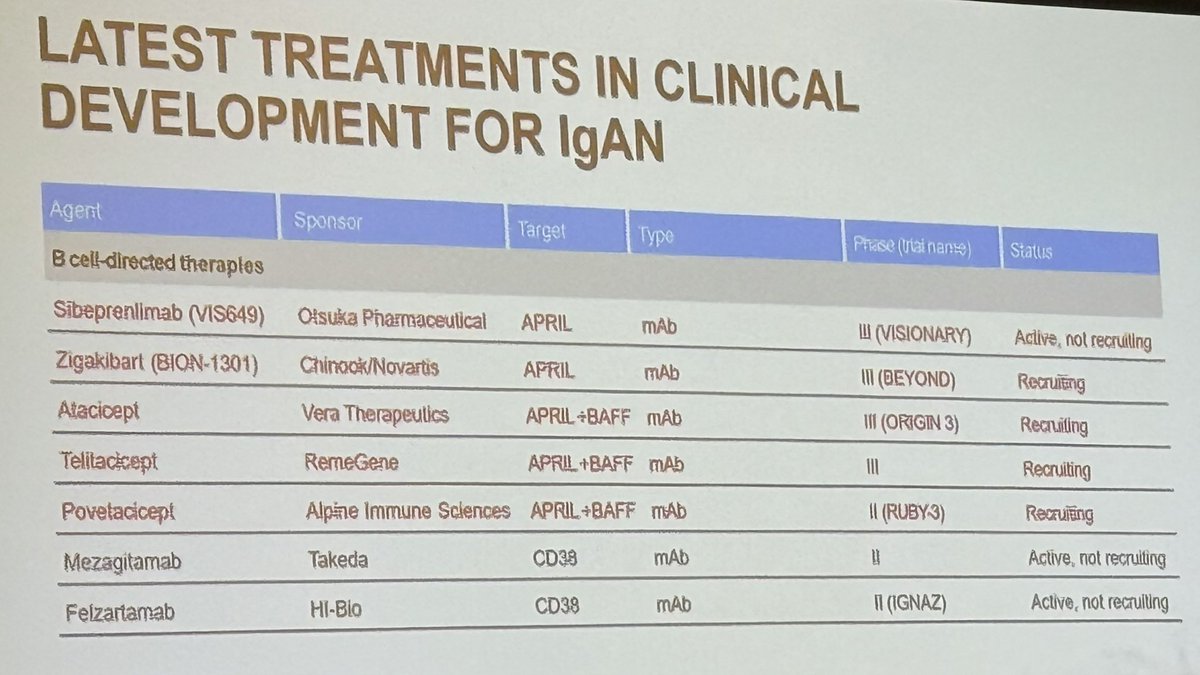
Dr. @fervenzafernan1 educating us on new treatment strategies in IgA nephropathy; & reminding us that just like proteinuria, hematuria is a good marker of disease activity and should be included in evaluating patient outcomes! 💯 @ASNKidney#KidneyWk ✨
@kidney_boy Not *statistically* significant but attending physicians (i.e., the control group) seems to have done a better job than the study team for the intervention group...
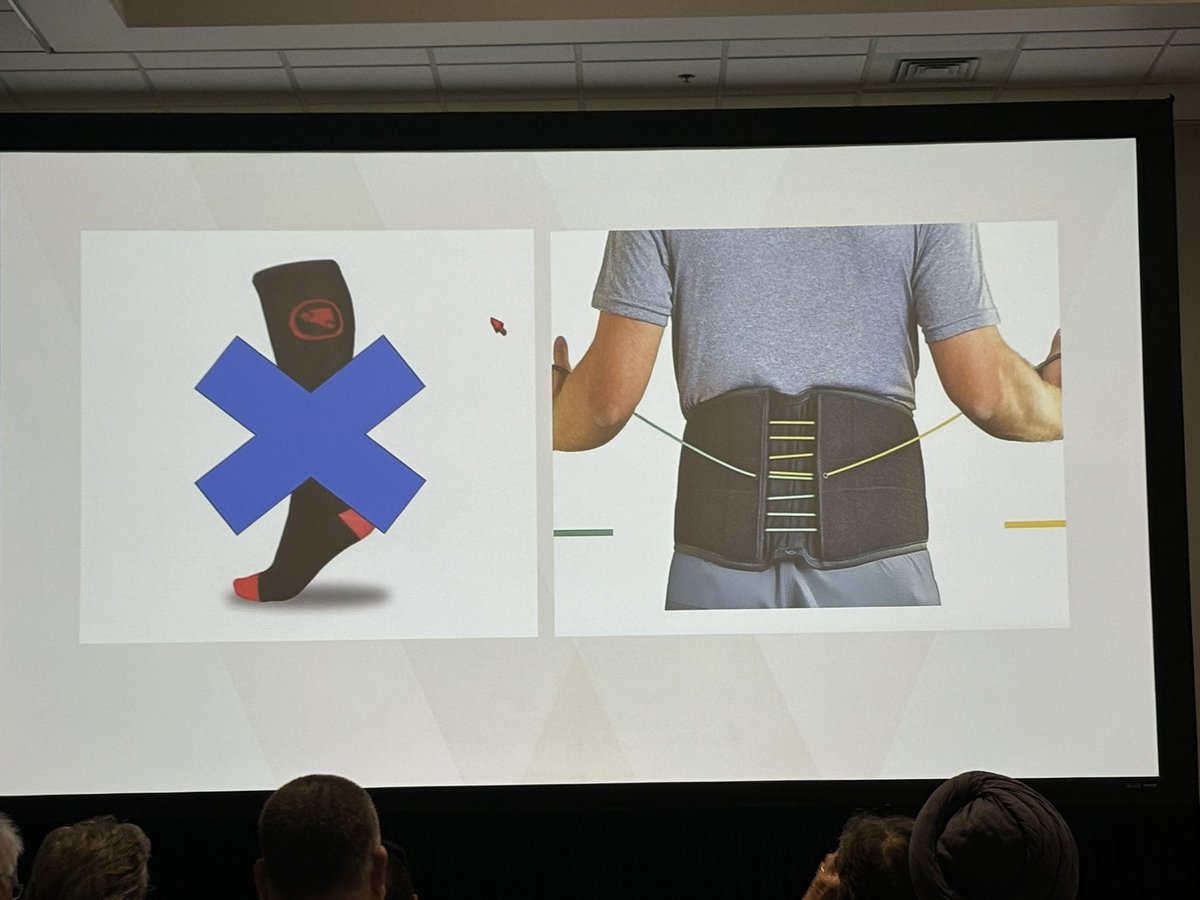
Abdominal banding more effective than compression stockings because it addresses the major standing venous blood pooling. Learned a lot on this lecture by Dr Shibao @VUMCDiscoveries#KidneyWk
Excited to share our latest publication on cause-of-death reporting in dialysis patients, comparing the US Renal Data System vs. the National Death Index. Important findings with implications for clinical practice and research👇: https://t.co/oBDLhv1SYI #dialysis#epidemiology
🚨Sharing our manuscript on Pantoea Peritonitis in Peritoneal Dialysis led by superstar fellow Dr. Brian Monk @UNCKidney and @Yoshi_Obi@UMMCMedicine
https://t.co/smwpHayiXA
@hswapnil@ManjulaKTamura So my understanding is that if you start HD in age of 70's, you may extend your life a bit and have a bit more days not on HD, but it would be counterbalanced by days for hospitalization, likely due to HD-associated complications like CLBSI, followed by SNF/NH/Rehab care.
@hswapnil@ManjulaKTamura I think there are two major contributors driving no meaningful difference between the two groups.
1. among the continued medical management group, 49% switched to dialysis within 3 years.
2. home time was the number of days ... not receiving inpatient care, SNF, NH, or rehab.
@osamaelshamy88 The NKF tried to address it a decade ago.😁
Top 5 Myths About Kidney Disease
"#1. I have back pain so it must be my kidneys."
https://t.co/RAd74NzH4x
@sarahkmels@askrenal In 1960s and 1970s when HD was not efficacious as it is now, uremic neuropathy could be prevented only with x3/week HD. It was clear to nephrologists without conducting clinical trials. Please check this out.
https://t.co/yF1bqs448B