Delighted to have won the
@RSMcoloproct
John of Arderne medal 🎖️ on my PhD researching metabolomic changes associated with radiation in locally advanced rectal cancer. Huge shout out to my supervisors @rickdunnblade@MSciacovelliLab & @dalevim for their support🚀🙏🧪😷!
Great talks at #SILASC by the #BRIDGES team yesterday
Huge shout out to @docdondons & @Mr_A_GT with some great research from their PhDs💥💥💥📚🤓👨🏽⚕️👩🏽⚕️
Organ Preservation and Survival by Clinical Response Grade in Patients With Rectal Cancer Treated With Total Neoadjuvant Therapy: A Secondary Analysis of the OPRA Randomized Clinical Trial | Oncology | JAMA Network Open | JAMA Network https://t.co/XIVIYUmCav
Important secondary analysis of the OPRA trial with a median f/u of 4 years.
This provides important details from a landmark study, and can help guide patient counseling. Of note, it's not broken down to compare induction TNT to consolidation TNT.
My analysis is long-winded, and the target audience is surgeons who offer organ preservation to patients with rectal cancer:
Patients with a cCR at restaging: 98% offered organ preservation/watch-and-wait (WW), of which 22% experienced local regrowth. Patients with a sustained cCR had a 5% rate of distant metastases.
Of the local regrowths, 93% underwent salvage TME and 7% underwent salvage local excision. For these patients, 33% developed recurrence (4% local, 22% distant, and 7% local+distant).
_______________________________________
Patients with a near-complete CR at restaging: 20 (17.5%) went straight to surgery, of which only 3 (16%) had a pathologic CR (pCR). Recurrence after upfront TME for near-cCR was 30% (15% local, 10% distant, 5% local+distant). These numbers were small (n=3 for local recurrence) and should be interpreted with caution.
Of the remaining 94 patients (82.5%) who underwent WW, 48 (51%) developed local regrowth. Salvage TME was performed in 34 patients (71% compared to 93% for cCRs). 2 of 34 TMEs (6%) had a pCR.
For patients with a near-cCR who developed regrowth after WW, 33% developed recurrence (4% local, 21% distant, 8% local+distant).
Of the 46 patients (40%) with a near-cCR who remained in the WW program, 13% developed distant metastases (compared to 5% for cCRs).
______________________________________
Patients with an incomplete response at restaging:
88% were offered upfront TME, of which 4/51 (8%) had a pCR. For ICR and upfront TME, recurrence rate was 35% (3.5% local, 21% distant, 10.5% local+distant).
8 patients with incomplete response were still enrolled in WW for different reasons, of which 5/8 (63%) developed local regrowth. All 5 underwent TME, and the local recurrence was 20% (1/5). Of the 3/8 that remained in WW without regrowth, 2/3 (66%) developed lung metastases.
_______________________________________
Overall, the 3-year organ preservation rate was 77% for cCRs and 40% for near-cCRs. The median time to TME for near-cCRs was 1 year.
3-year DFS was 88% for cCR, 69% for near-cCR, and 56% for incomplete response.
_____________________________
For patient counseling purposes:
Of the 123 patients with a cCR who were offered WW, the local recurrence rate was 22% (0f which 93% underwent salvage TME) and the rate of distant metastasis was 10.5%.
Of the 94 patients with a near-cCR who were offered WW, local recurrence rate was 51% (of which 71% underwent salvage TME) and the rate of distant metastasis was 15%.
Of the 57 patients with incomplete response who were offered upfront TME, local recurrence was 14% and the rate of distant metastasis was 32%.
@JohnRTMonsonMD@R_Perez_MD@ianmpaquette@JonVogel7@jendavidsmd@KyleCologne@debby_keller@juliomayol@Neil_J_Smart@FergaljFleming@ScottRSteeleMD@JISBMD
Happy 2024! Thrilled to share that my first-author paper, stemming form my PhD project, has been published @JMolBiol. Feel free to reach out for any questions. Thank you to my supervisors for helping out and making this possible.
https://t.co/5eoAQcAH6G
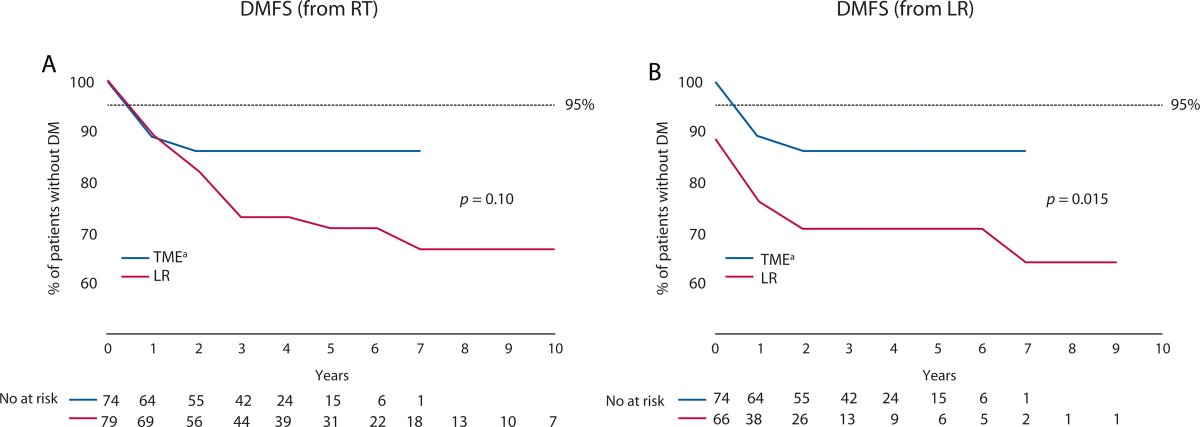
Is the risk of distant metastasis higher in those rectal cancer pts undergoing surgery for local regrowth compare to those undergoing upfront surgery for near complete response after chemoradiation? Find out in #DCRJournal: https://t.co/SjMTBdoL7W
@Swexner@me4_so@ACPGBI
Just saw this rectal cancer study in @JAMAOnc – lots to digest.
Despite absolute 50% drop (87% to 37%) in use of neoadjuvant RT for lower risk (cT1-3, N0-1, MRF-) rectal cancers from 2011 to 2016, no difference in local recurrence & survival improved.
https://t.co/fbjPyAvATu
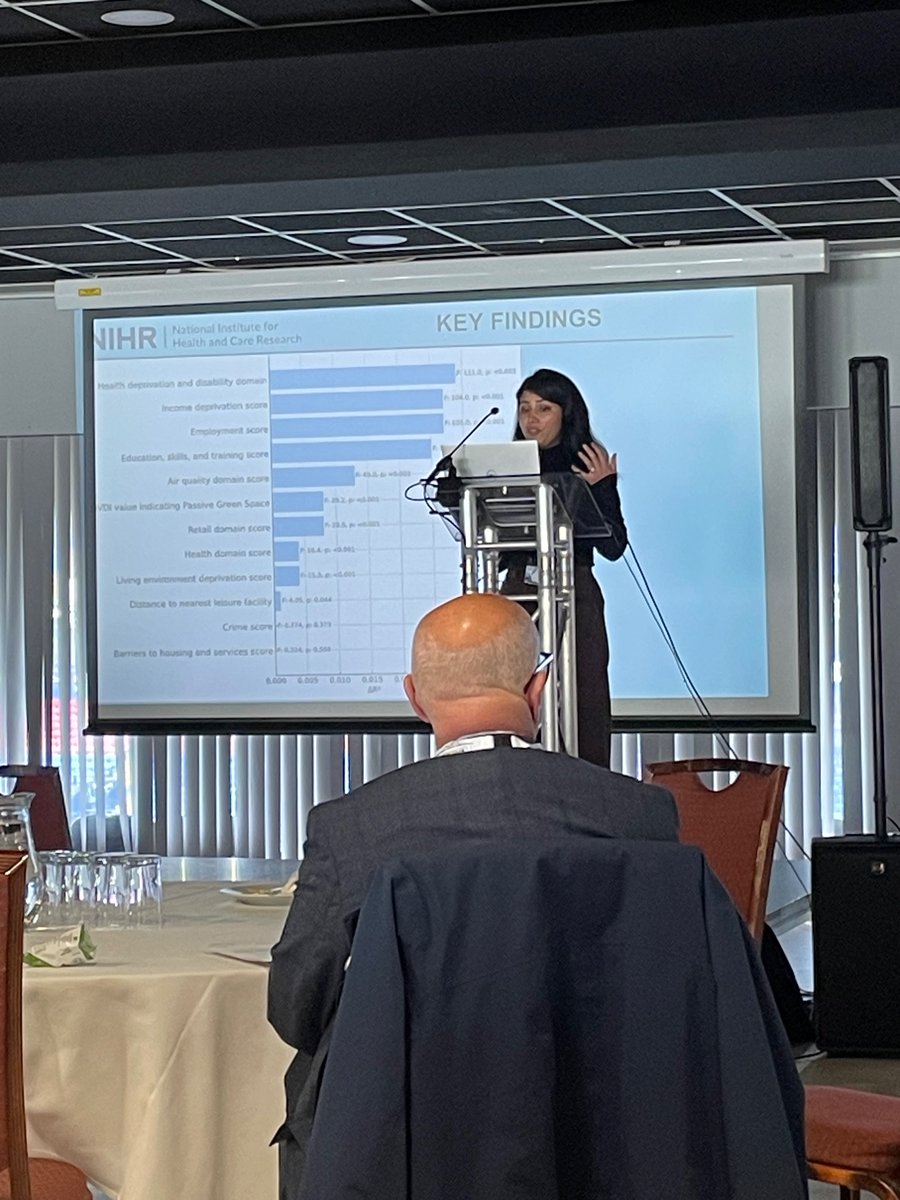
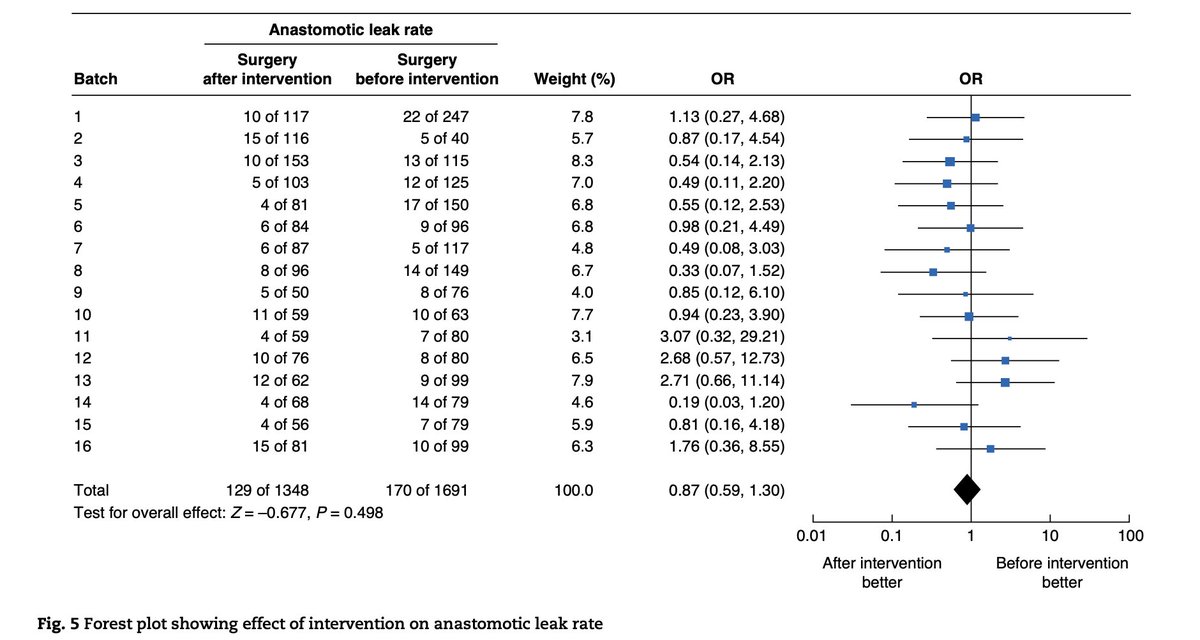
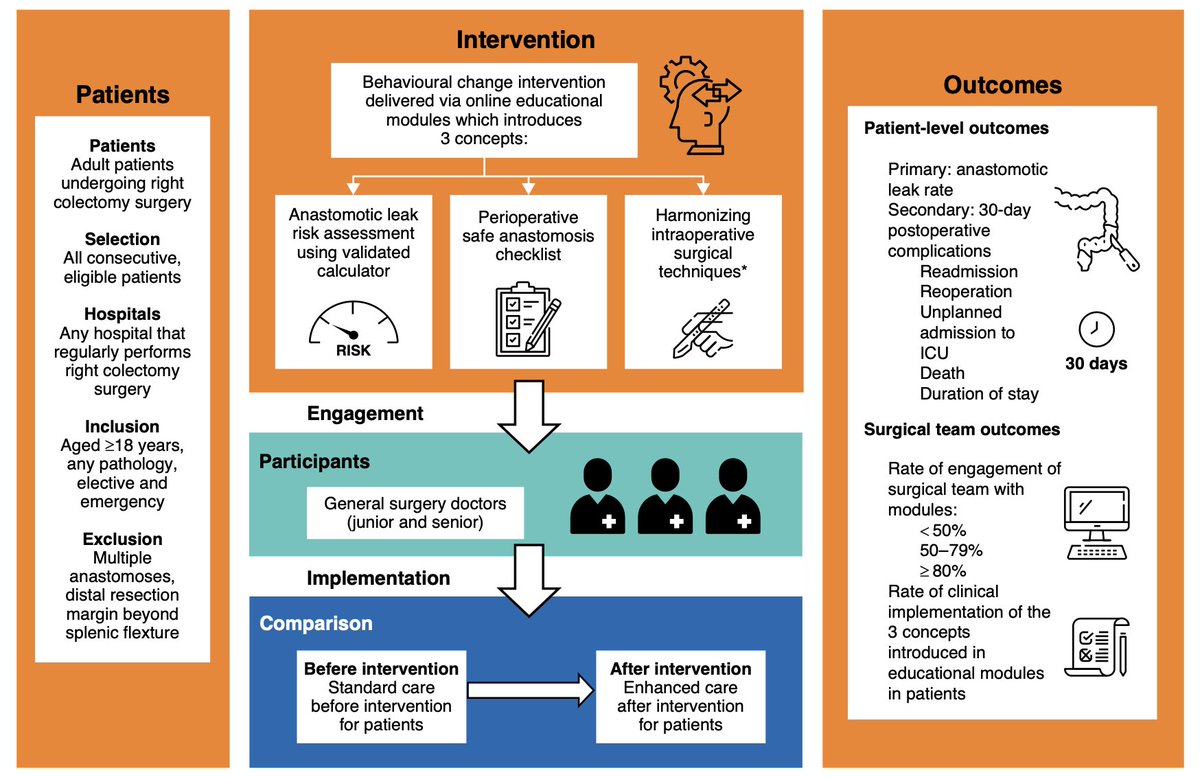
🔥The EAGLE study is out!
Evaluation of a quality improvement intervention
to reduce anastomotic leak following right colectomy
(EAGLE): pragmatic, batched stepped-wedge,
cluster-randomized trial in 64 countries
➡️ https://t.co/pDfy4r6k9R
By the ESCP EAGLE Safe Anastomosis Collaborative and NIHR Global Health Research Unit in Surgery
🏥 332 participating 💪 Great collaborative work!
Outcomes:
1⃣ The absolute anastomotic leak rate was 10.1 per cent (170 of 1691) during data collection before the intervention and 9.6 per cent (129 of 1348) in the data collection interval after the intervention.
2⃣ Confidence intervals for intervention effects on secondary outcomes were wide but ruled out reductions of more than 40% in the odds of death, readmission, reoperation, unplanned ICU admission, stoma without primary anastomosis, and longer hospital stay.
The EAGLE trial did not find conclusive evidence for a reduction in anastomotic leak rates following the intervention, although a subgroup analysis did identify a reduction in leak rates in hospital teams with high team engagement in the intervention. This may reflect better knowledge, better decision-making, and more engaged team performance through enhancement of non-technical skills.
@EagleEscp@escp_tweets@YouESCP #SoMe4Surgery #MedTwitter #SurgEd #Surgery #colorectalsurgery #StepUp4CRC @FightCRC@BjsOpen@BJSAcademy@ESCP_studies@NIHRresearch@ACPGBI@ACPGBI_EduTrain@Dukes_Club@NIHR_GSU
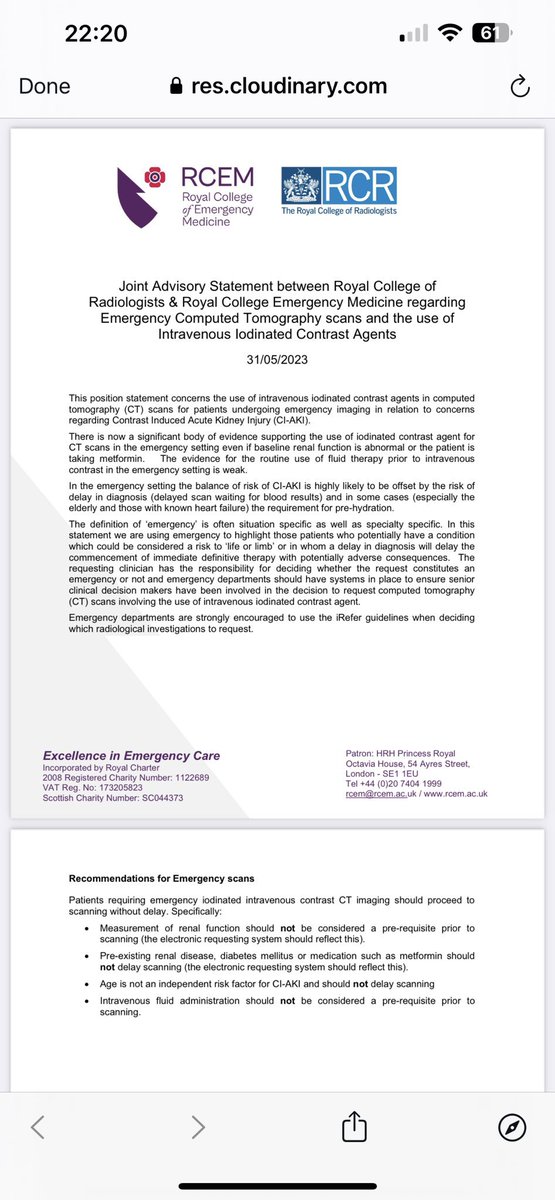
I remember some radiologists asking for my GMC number and asking me to type on the request “I take responsibility if contrast causes AKI” as a F2, to get a contrast CT scan done.
It’s taken a long time despite the evidence being there for years.
I’m shocked Junior Doctors are on a £14 hourly wage? I find that mind blowing, considering I wasn’t far behind that teaching Boxercise classes in the early noughties. Are you shocked by this? The Dr’s pay that is, not the Boxercise? #JuniorDoctorsStrike