Our latest review on post-transplant malignancy is now published. Grateful to @iamnephrologist through @ISNkidneycare Mentorship Program for the mentorship and support that brought this work to fruition. VA @nyiminhan
Our latest review on post-transplant malignancy is now published. Grateful to @iamnephrologist through @ISNkidneycare Mentorship Program for the mentorship and support that brought this work to fruition. VA @nyiminhan
@mikeachimugu01 , thank you for your intervention as I have received my compensation from @TurkishAirlines . This could not have been possible without your leadership and the professionalism of the @NCAA team.
Why is it that evil keeps befalling your friends?
If it’s not stroke today, it would be MI, it would be splenic rupture
And one theme is : No ECG, No CT, no this, no that.
Won fi se e ni
1/Hello everyone!Ebola on the agenda today
Welcome to a deep dive into the renal realities of Ebola Virus Disease (EVD).
*⃣Nephrologists, grab your coffee, this thread is for you. #MedTwitter#NephTwitter#MedX#Ebola
🔆Need to standardise HDF practice & promote wider adoption across 🇮🇳 subcontinent
🔥survival benefit, lower CV complications, lower IDH, better QOL
🔗 https://t.co/C9fCdDxs4N
🧵 1/5
⚖️ ETHICS Committee Workshop: Between a Rock and a Kidney Conundrum
🎤 Lecture 1: Approaching “Disruption” and “Non-Adherence”
👤 Simon Sawhney & Gulcin Kantarci
💡 The session challenges us to move beyond labels such as “non-adherent” and “difficult patient” and instead explore the underlying barriers, circumstances, and values influencing patient behavior.
🤝 Ethical kidney care starts with understanding before judging.
📍 #ERA26
😕Sadly, but happening now closing lectures
🤩the exciting part is Plenary Lecture - From Science Fiction to Reality: The Xenotransplantation Revolution by @LVRiella
👇Since the first kidney transplant in 1954, long-term success remains limited by rejection, disease recurrence, and organ shortage
🔬Research focuses on immune tolerance, preventing recurrent disease, and expanding the donor pool through xenotransplantation
#ERA26
Next from hall 3b, open you mind session
@KatherineTuttl8 talking about aldosterone synthase inhibition (ASI) for treatment of CKD #ERA26
📍 Inflammation and fibrosis are key final drivers of CKD progression
📍Aldosterone promotes kidney and cardiovascular injury beyond BP effects
📍MRAs target these pathways, but hyperkalemia limits use
📍Potassium binders may enable safer MRA therapy
🔥During #ERA26 Late-Breaking Clinical Trials 2, @AgarwalRajivMD presented efficacy and safety of finerenone in patients with chronic kidney disease: a pooled individual participant data analysis (INFINITY)♾
Finerenone trials included a broad CKD population encompassing a range of disease aetiologies and levels of glycemia, eGFR & albuminuria
1/7 🧵 #ERA26 - High impact clinical trials in Nephrology. #ChallengeYourThinking
🪑: Mario Gennaro Cozzolino @MarioCozzolin19; Kaitlin Mayne
Ravulizumab in IgA nephropathy: a prespecified interim analysis of the phase 3 I CAN trial. Promising complement-targeted data in IgAN.
💬: Jonathan Barratt @IgAN_JBarratt
🔥High impact clinical trials in Nephrology #ERA26
⏩MOTheR HDx Study: A MOPR Study to Explore Morbidity and Mortality in Patients Dialyzed with Theranova HDx Compared with OL-HDF
🎙️Presented by @DePsequera
The evolution of dialysis during the last decades gets us nowadays to hemodiafiltration and to medium cut off membranes discussions
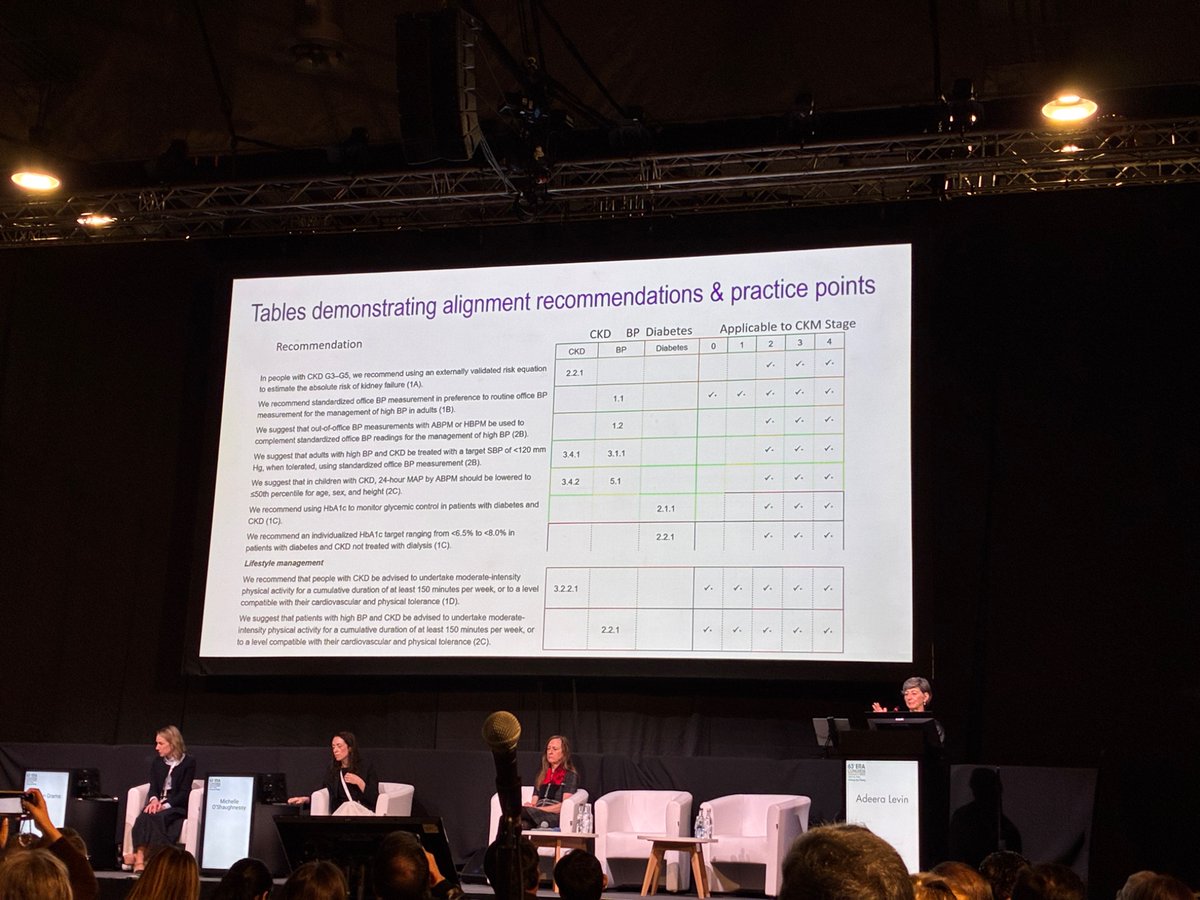
CKM Syndrome: "The Kidney in the Middle" | #ERA26
Adeera Levin at #ERA26 on KDIGO CKM Commentary: CKD is not just a kidney problem. It sits at the center of Cardio-Kidney-Metabolic syndrome, driving CVD risk and mortality.
CVD Burden in CKD is Massive
Prevalence climbs with CKD stage: No CKD 37.5% CVD prevalence → G2 63.4% → G3 66.6% → G4-G5 75.3%
Mortality skyrockets: Annual mortality risk highest in lowest eGFR + highest albuminuria. CKD patients have far higher CV death than general population, especially young patients with dialysis
KDIGO Risk Heatmaps: Predict 10 Outcomes
eGFR + uACR = risk stratification: Heatmaps from 27.5 million people show risk for 6 CV outcomes, 2 kidney-specific, 2 general outcomes by age, eGFR, albuminuria
Red zones = high risk: Lower eGFR G3b-G5 + higher albuminuria A2-A3 = red/orange. Predicts CV mortality, heart failure, stroke, MI, hospitalization, kidney failure replacement therapy
KDIGO Guidelines Address CKM Components
CKD definition is CKM entry: KDIGO defines CKD by kidney structure/function/urine abnormalities >3 months, staged by GFR + albuminuria
Guidelines cover CKM: KDIGO Clinical Practice Guidelines directly address CKD evaluation, blood pressure, diabetes management, lipid management. Upcoming guideline on heart failure in CKD
Overarching themes: Early detection/intervention + comprehensive personalized management + multidisciplinary care
Why Nephrologists Matter in CKM
Kidney role: Initiates, amplifies, and modifies severity/temporality of CVD/metabolic processes
Nephrologist role: Initiate diagnostics + therapies, amplify treatment based on risk, modify patient outcomes
Lifespan approach: KDIGO guidelines consider fetal-maternal health, sex, gender, regional/cultural differences, age for outcomes + applicability
Takeaway: CKD = CKM Stage 1+. Higher creatinine + albuminuria = higher CV risk and mortality. KDIGO risk heatmaps guide who needs aggressive prevention. Message: detect early, stage by eGFR + albuminuria, manage comprehensively with nephrology + cardiology together.
Presentation: Adeera Levin | Tweet: @eroldemir83 on behalf of SoMe Team
🔥Last presentation in high impact clinical trials in Nephrology #ERA26
⏩Efficacy and Safety of SGLT2 Inhibitors in Alport Syndrome: A Multicenter Prospective GLIFAS Study
🎙️Presented by Domenico Santoro
🧬Alport syndrome results from COL4A3–5 variants affecting GBM collagen
KDIGO 2026: New Paradigm for Diabetes + CKD - Prevent, Don’t Just Treat | #ERA26
Forget single-drug thinking. KDIGO 2026 guideline shifts to comprehensive, personalized, early combination therapy for diabetic CKD. Katherine R Tuttle broke it down.
2026 KDIGO Guideline Paradigm
3 principles: Personalized, accelerated, iterative therapy
4 pillars: 1) Lifestyle: diet, exercise, weight, smoking cessation 2) Foundational pharmacotherapy: SGLT2 inhibitor, statin, RAS blockade 3) Additional risk-based: nsMRA, GLP-1 RA, antiplatelet 4) Treatment targets: BP, lipids, glycemic control
Risk Stratification: Know Your Zone
KDIGO heat map: Risk by eGFR G1-G5 + albuminuria A1-A3. Red = high risk G3b-G5 + A2-A3 → "Treat and refer"
Goal: Move patients from red to yellow/green zones early with multifactorial intervention
2026 nsMRA Update - Finerenone
New 1A recommendation: Add nonsteroidal mineralocorticoid receptor antagonist with proven kidney/CV benefit for T2D + eGFR ≥25 milliliters per minute per 1.73 square meters + normal potassium + albuminuria ≥30 milligrams per gram while on max RAS inhibitor
Combo strategy: For persistent albuminuria on RASi, SGLT2i + nsMRA can be initiated simultaneously to mitigate hyperkalemia risk
Combination Therapy = Additive Protection
Kidney + CV outcomes: Adding to RAS blockade, each drug class helps. SGLT2i, GLP-1 RA, nsMRA. Triple combo SGLT2i + GLP-1 RA + nsMRA gives lowest HR for CKD progression 0.42, MACE 0.65, heart failure hospitalization 0.45
Finerenone + Empagliflozin: CONFIDENCE trial showed 52 percent albuminuria reduction at 180 days with combo vs 29 percent empagliflozin alone, 32 percent finerenone alone
Takeaway: KDIGO 2026 says "Yes, we CAN prevent CKD in diabetes". It’s not about one drug. It’s glycemic control + BP control + lifestyle + SGLT2i + GLP-1 RA + nsMRA + RAS blockade, started early and adjusted iteratively. Risk-based, not one-size-fits-all.
Presentation: Katherine R Tuttle | Tweet: @eroldemir83 on behalf of SoMe Team
Happening in Clyde now at #ERA26
Prediction, precision and inclusion in ANCA vasculitis: open your mind to new possibilities
Should steroids take a back seat in 2025: real world use of avacopan
🗣️Lorraine Harper
MAJESTY trial #ERA26@ERAkidney
Obinutuzumab >>tacrolimus in primary MN
✅ ⏫complete remissions
✅ ⏫reductions in proteinuria
✅ ⏩ faster and more sustained anti-PLA2R remission
✅ ⬇️relapse and need for rescue therapy
✅ ⚠️Acceptable safety profile