R-E-S-P-E-C-T 🎵
The #QueenOfSoul didn’t just ask for it — she demanded it, lived it, and helped redefine it for women everywhere.
#OnThisDay, we remember Aretha Franklin, who inspired millions with her music and activism.
Her legacy lives on 🎶
#ArethaFranklin
🤬 Backlash is organized.
⛔ Rights are being reversed.
🚫 Impunity is spreading.
Women and girls have never been closer to #equality.
And never closer to losing it.
See why #IWD2026 is our collective moment for action: https://t.co/sfJVVPAl39
#ForAllWomenAndGirls
When people accept the unacceptable, it quietly becomes acceptable.
And that, to me, is the most unacceptable thing of all.
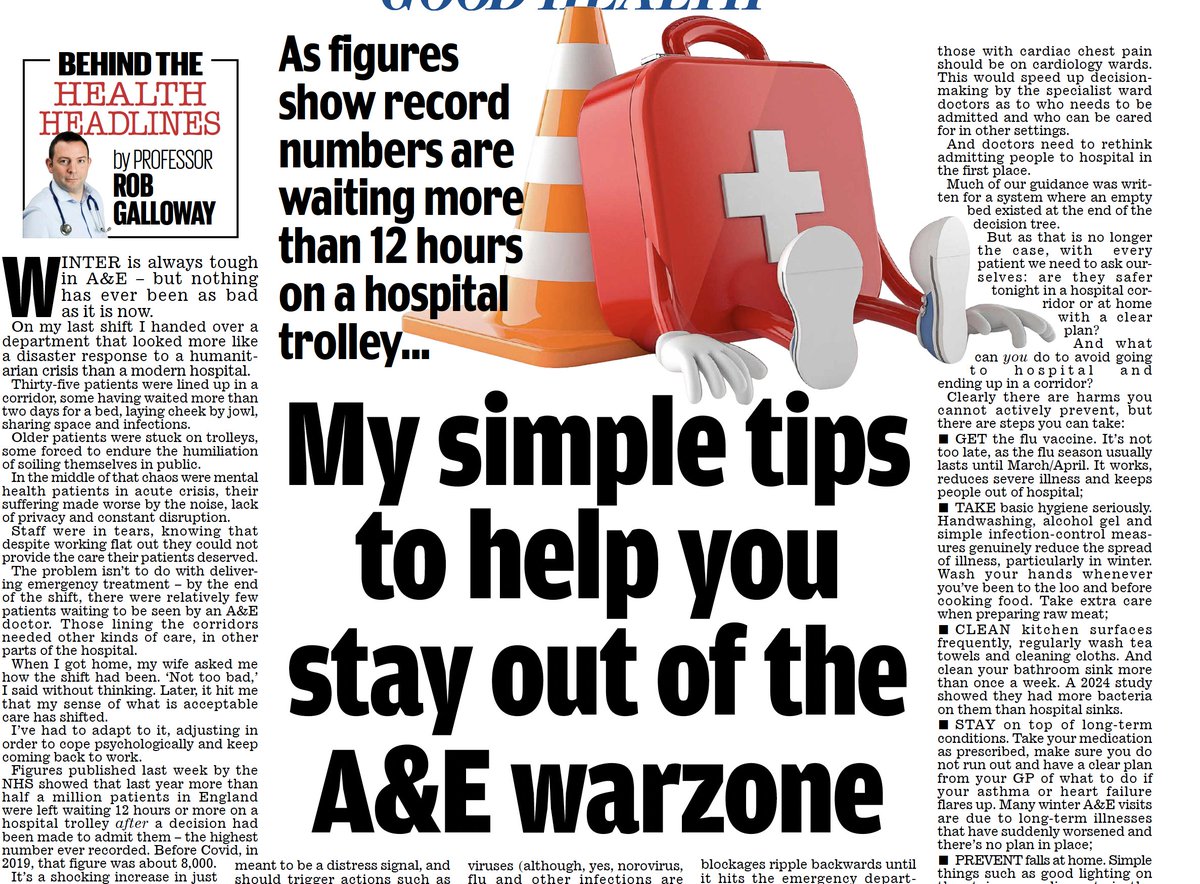
Right now, in A&E departments across the country, patients who should be in proper hospital beds are being cared for in corridors. This isn’t a rare emergency measure. It isn’t a winter-only phenomenon. It isn’t a sign that “things are stretched today”.
It is normal practice. In my latest article for the Mail Health section I explain the reality of what is actually happening in A&E departments. Its truly awful…..
Older patients lie on trolleys for days. Frail people wait without privacy, dignity or rest. Some soil themselves in public. People with dementia or delirium become more confused. Patients with mental health crises sit in noise and chaos that actively worsens their distress. Infections spread. Pain goes untreated for longer than it should. Families watch, helpless and shocked.
And yet, outside the hospital walls, almost nobody notices.
That is what frightens me most.
Inside A&E, staff are working flat out. They are not lazy. They are not indifferent. They are doing everything they can to deliver safe care in a system that no longer allows it. I have seen experienced, resilient clinicians cry at the end of shifts. Not quietly upset, but broken by the feeling that they are participating in something unsafe and degrading despite their best efforts.
But here is the uncomfortable psychological truth: to survive, we adapt.
You come home after a shift like this and someone asks how work was. You say, “Not too bad.” And you mean it. Because if you let yourself fully feel how bad it really was, you wouldn’t be able to go back the next day.
Your internal bar for what counts as acceptable care quietly drops.
Once that happens, the system stops screaming. Corridor care stops being a scandal and becomes background noise. “Critical incidents” lose their meaning because the pressure is no longer exceptional – it is constant.
And because this suffering is largely hidden inside hospitals, it slips out of the news cycle. No dramatic single event. No clear villain. Just a grinding, everyday erosion of standards that would once have been unthinkable.
The truth, which we need to say out loud, is this: A&E is not coping. The situation is not meaningfully improving. And comforting narratives about “recovery” do not match what staff and patients experience on the ground.
If we want this to change, three difficult things have to happen.
First, we have to change how the NHS is run.
This is no longer simply a funding argument. The NHS is receiving more money than it ever has. But it is using that money badly, and in the wrong places. We have built a system obsessed with hospitals, expensive interventions and downstream fixes, while hollowing out the parts of the system that prevent people needing hospital care in the first place.
We are losing experienced generalists – particularly GPs – who know their patients, understand risk, and can safely manage uncertainty in the community. They are being replaced by less experienced doctors working under impossible pressure, with fewer appointments and less continuity.
In that environment, risk is pushed uphill. Patients are referred to hospital “just in case”. And once someone crosses the hospital threshold, everything becomes harder. Beds don’t exist. Discharges are delayed. Social care isn’t there. Those blockages ripple backwards until they hit A&E, where the pressure finally becomes visible as corridor care.
If we are serious about fixing A&E, we have to stop pretending hospitals alone can absorb unlimited demand. Investment has to move upstream. Community care has to work. Care packages need to be available in hours, not weeks. Experienced clinicians need to be retained, not driven out.
Second, we have to change how doctors think about risk.
This is deeply uncomfortable for the profession, but unavoidable. Much of our clinical guidance was written for a system where an empty bed existed at the end of the decision tree. That assumption is now false.
Doctors are already doing everything they can to avoid admitting patients to hospital, not because they are negligent, but because admission itself has become risky when patients are destined for corridors rather than wards.
We now have to ask a brutally honest question with every patient: are they safer tonight in a hospital corridor, or at home with a clear plan, safety-netting and follow-up?
That feels wrong. It goes against decades of training. But pretending that hospital is always the safest place is no longer true when the system is overwhelmed. This requires courage, honesty with patients and families, and a shift away from defensive, default admission that the system can no longer sustain.
Third, we have to be honest with the public about what patients themselves can do.
This is not about blame. It is about realism. Overwhelmed hospitals are dangerous places. There are harms you cannot control, but there are things people can do to reduce their chances of ending up in A&E in the first place.
In my latest article for the Daily Mail health section, I set these out clearly. Get vaccinated. Take basic hygiene seriously. Manage long-term conditions properly and have a clear plan for flare-ups. Prevent falls at home. Go easy on alcohol. Keep simple medications at home. Think carefully before defaulting to A&E when safer alternatives exist.
And crucially, if a doctor says a relative needs to stay in hospital, it is reasonable to ask why. If the reason is simply waiting for tests or reviews, it is fair to ask whether this could be done safely as an outpatient instead.
None of this is easy to hear. None of it fits neatly into slogans or soundbites.
But honesty is not disloyal. It is not anti-NHS. It is not pessimism.
Honesty is the only route to change.
Silence is how the unacceptable becomes normal.
And once that happens, it becomes very hard to remember that it does not have to be this way.
https://t.co/q2MCX8nSJa
Dear African healthcare worker (some-this is not discrimination but lived experience)!
If you’re going to be a nurse or HCA, at least exhibit the values and ethics of the organisation you’re representing! Unprovoked bad behaviour is UNACCEPTABLE! cc: #KingsCollegeNHS
@sandikrakowski Today, I am grateful for Sandi! I spent 2 and half years learning and it’s paying off! I never would have known so much about the markets without her insights! Honor where it’s due! ❤️
👋
Would you please consider giving a #gift to a #child or a family?
I’ve been with Compassion for 10 years & they do what they say.
Proverbs 22:9.The generous will themselves be blessed, for they share their food with the poor.
https://t.co/enddJXKUAD https://t.co/enddJXKUAD
« Les choses, il faut bien les faire ! »
En présence du Chef de l’Etat, @Fatshi20/@fatshi13 et la distinguée Première dame, @DeniseNyakeru,
Pour les obsèques du Patriarche @JPKambila, j’ai eu la lourde charge de présider la cérémonie et prononcer l’oraison funèbre.
Paix à l’âme de l’illustre disparu 🕊️
2 legends gone… Former NBA star, Mutombo Dikembe 🇨🇩🇺🇸and former Deputy Chief of Staff to President 🇨🇩, my older sister’s dad, Uncle Jean-Pierre Kambila🇨🇩🇨🇭…
Rest well Tonton 😢💔