In medial achilles tendinitis which have a compressive plantaris component, hydrodissection or “stripping” of the plantaris tendon under US can help remove painful adhesions.
You can then trace plantaris proximally up to the MTJ to see it has been dissected away properly.
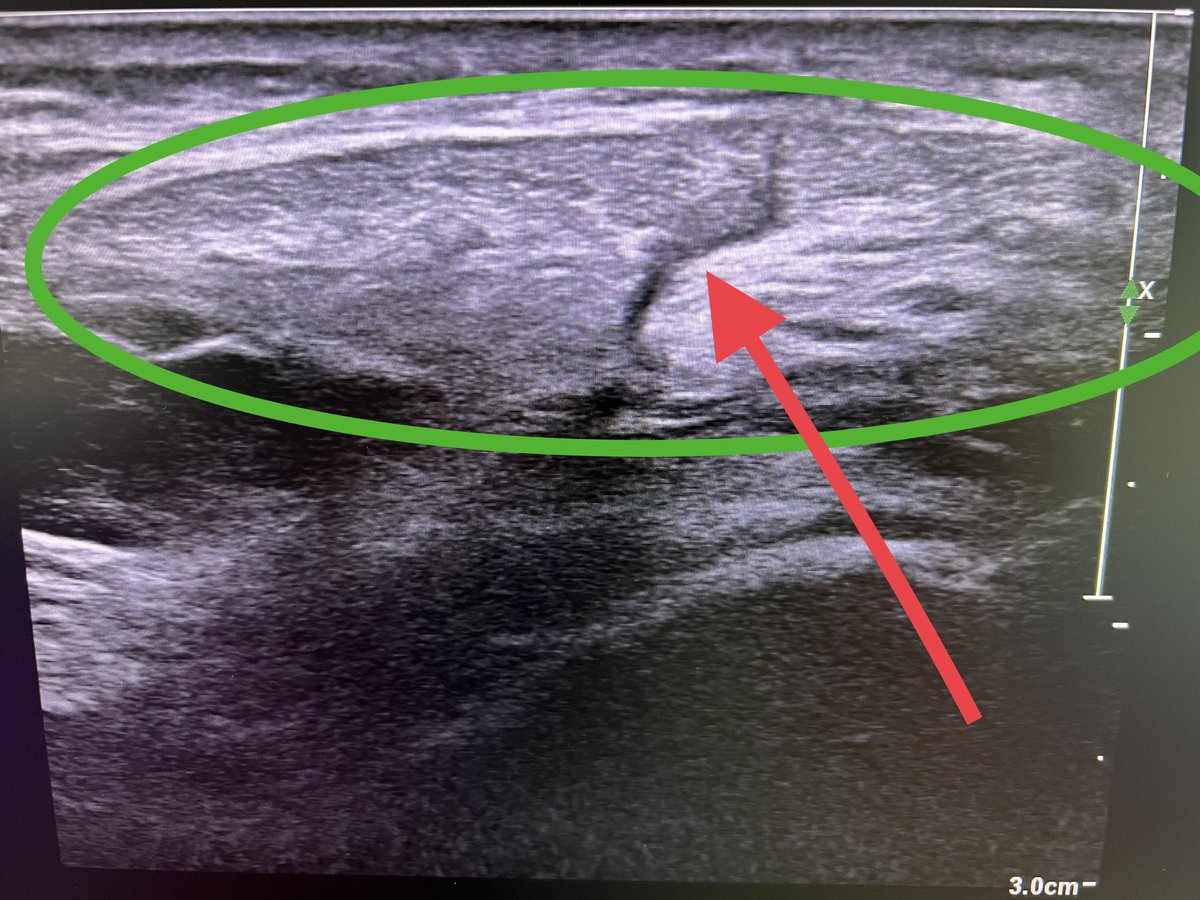
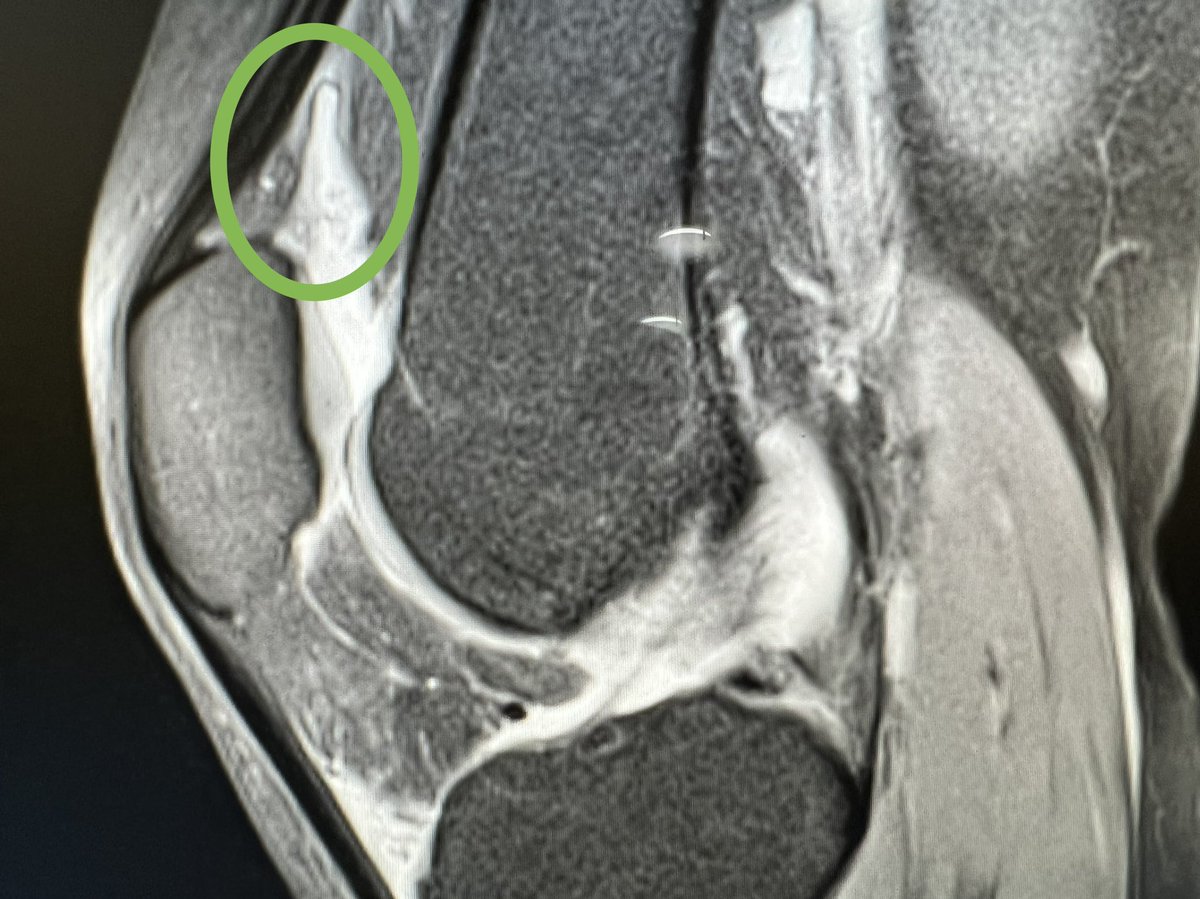
Seen a few patients post knee arthroscopy where a port has been put through the patella tendon (green oval) causing scarring (red arrow) pain, poor quad functx.
Any advice on how to avoid this from our knee surgeons?
Difficult to estimate width of PT from palpation alone.
Another case of transient bone marrow oedema of the foot in a runner.
Specific lower limb and foot DEXA can be very useful here
The problem is there is no large comparative data set to calculate meaningful SD scores and won’t be until we start scanning more
Chicken and egg!
A case of Parson Turner syndrome after “aggressive” soft tissue treatment in the neck and shoulder area. Patient developed acute neuropathic pain post treatment and subsequent right upper girdle wasting.
A reminder not to go prodding too vigorously in the triangles of the neck?
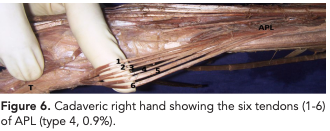
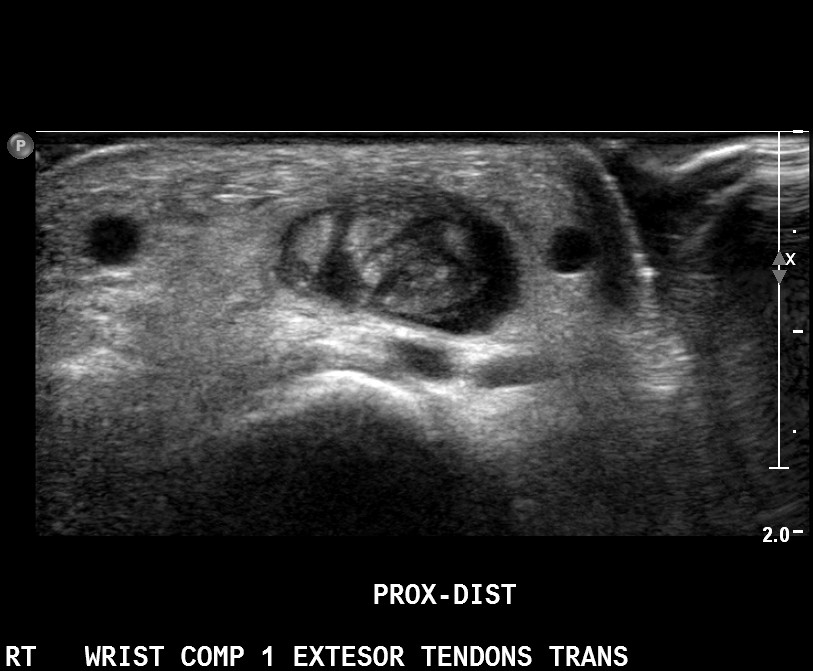
De quervains and 1st extensor wrist comp pathology is often over diagnosed on ultrasound. APL can have multiple strands, up to 6! Which can look very busy on ultrasound scanning.
The more strands, the more likely there is to be friction between them and be symptomatic.
Hi all,
Hoping to collect for SportsAid this RideLondon2023. A great charity supporting young athletes, i'm sure those in SEM have heard and interacted with them before. Any donations welcome! 🙏
https://t.co/RLsX5yDYNz
Free webinar discussing the latest concepts in Groin and Pelvic floor issues in sport, hosted by London Bridge Sports Medicine.
18th April 18-1930pm, CPD points awarded!
Would be great to have you there!
Click on the link below to register👇
https://t.co/2bhW3KUux0
A less common cause for plantar pain, plantar cysts. Arise from the MTPJ and often misdiagnosed as metatarsalgia or plantar plate injury.
Look out for in anyone with tenderness on the MTPJ head and the plantar side, and pain on plyometrics.
These can be easily drained.
We’re pleased to share that Dr @ajaiseth Consultant in Sport, Exercise and Rehabilitation Medicine has joined the ISEH.
To learn more or to enquire about an appointment, visit:
https://t.co/NQpYY9Y6hL
#adolescentsportsmedicine
The two virtual evenings in the ISEH conference series taking place soon are:
✅Adolescent Sports Medicine *Monday 30th January 2023*
✅Tendinopathy and Tendon Tears *Tuesday 31st January 2023*
It’s free to attend our CPD accredited conference series: https://t.co/qt1ZYK3xOx
Rice bodies in joints can cause mechanical Sx (e.g locking, crepitus) as well as functional Sx (apprehension, instability).
Usually a sign that there has been previous synovial inflam from inflam diseases or infection.
If anyone has nice pics of them on US please share!
Shoulder Muscle lesions can act as a good predictor for cervical nerve entrapments.
This patient has supraspinatus wasting and fatty infiltration resulting from a C5 nerve root impingement (thus affecting suprascapular nerve). Also complains of general shoulder aching.
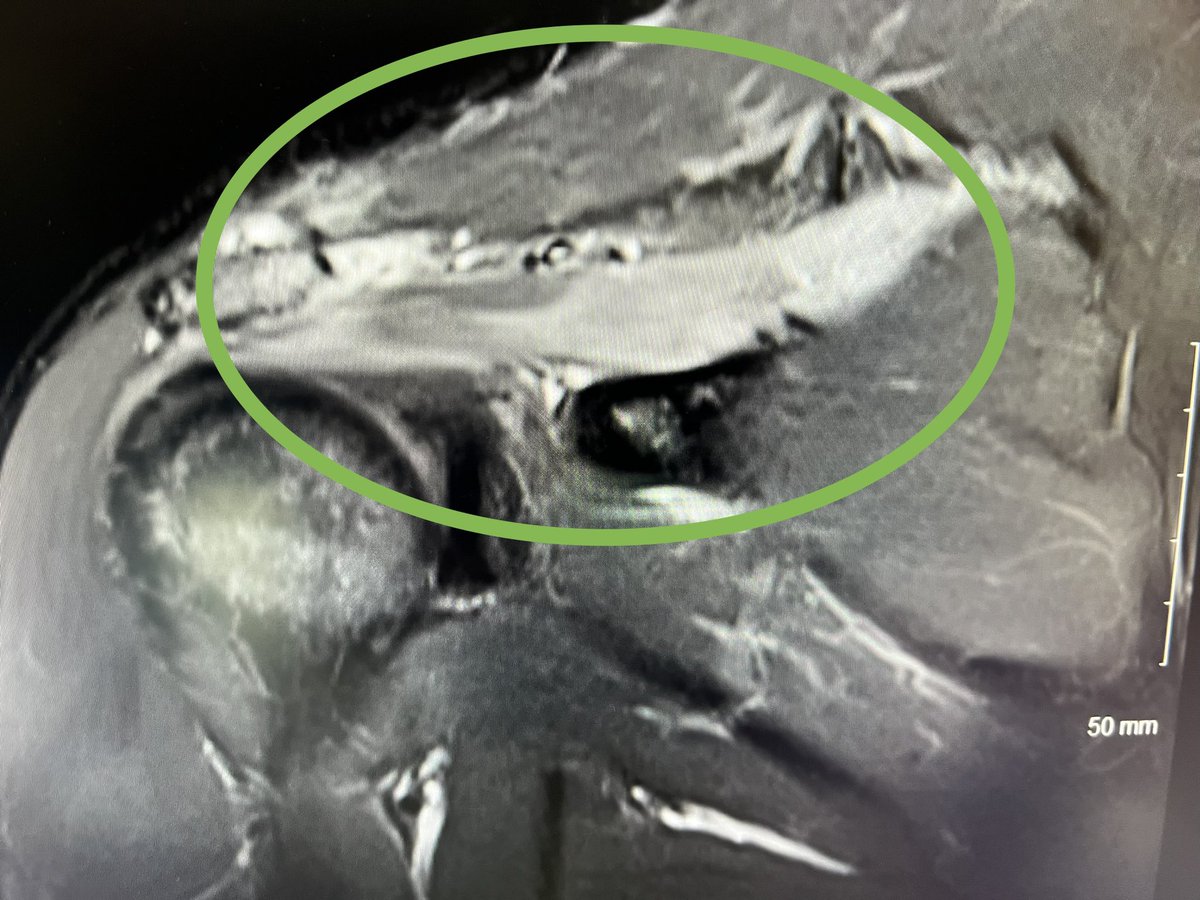
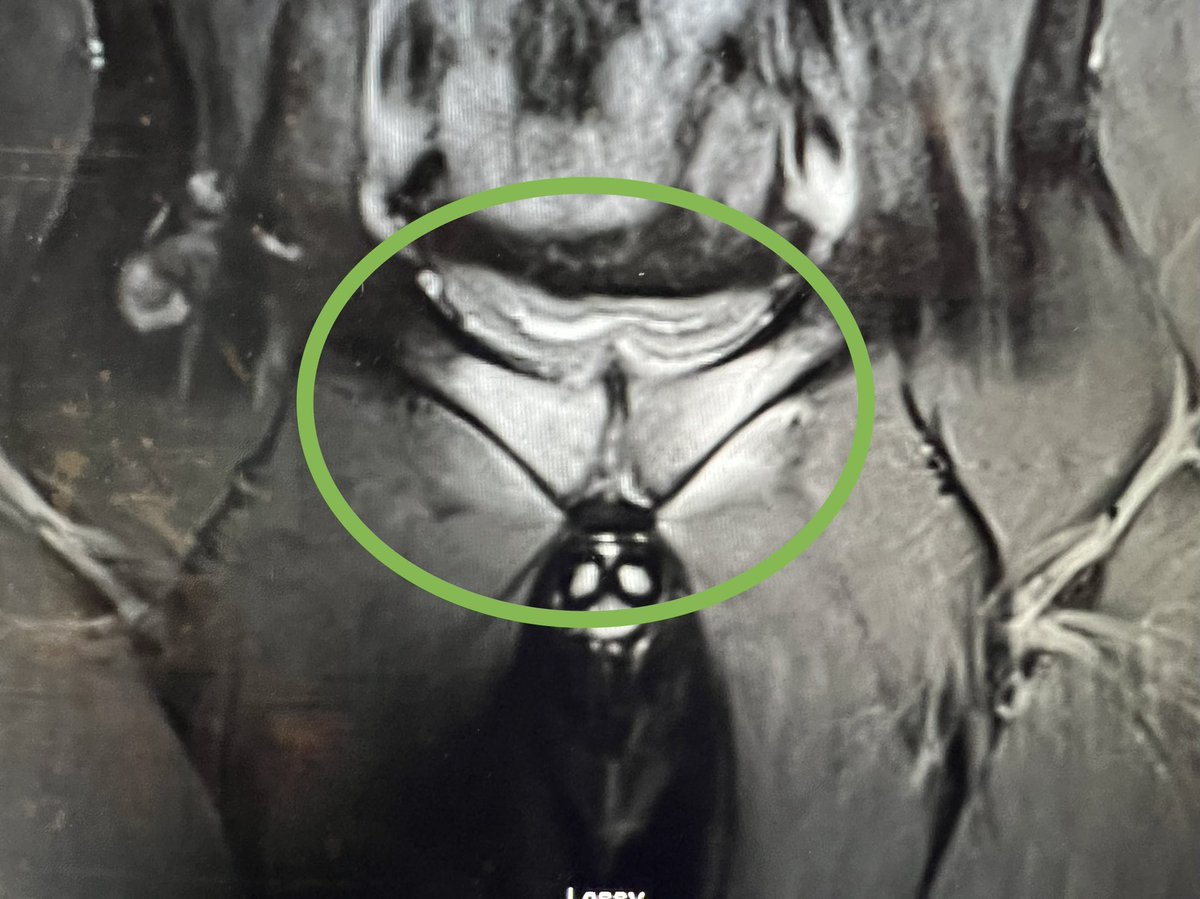
Florid pubic and rami bone oedema in a footballer in his 20s, male. I was asked to exclude sportsman’s hernia.
Loading and training history essential and identify any other risk factors eg dietary changes, weight loss/gain.
Can often predict level of overload from Hx and Ex.
Cross section view of a retrocalcaneal bursa.
Certainly a pain generator in its own right when this inflamed and usually associated with insertional TA tendinopathy but not always.
Palpate around base of tendon and over the RC bursa. DF of step usually provocs too.
No need to duplicate imaging! This Weight bearing x-Ray tells you all you need to know about this 63 year old patients knee arthritis. MRI doesn’t add any additional information plus doesn’t have the advantage of being weight bearing.
He had been referred for both! 🤦🏽
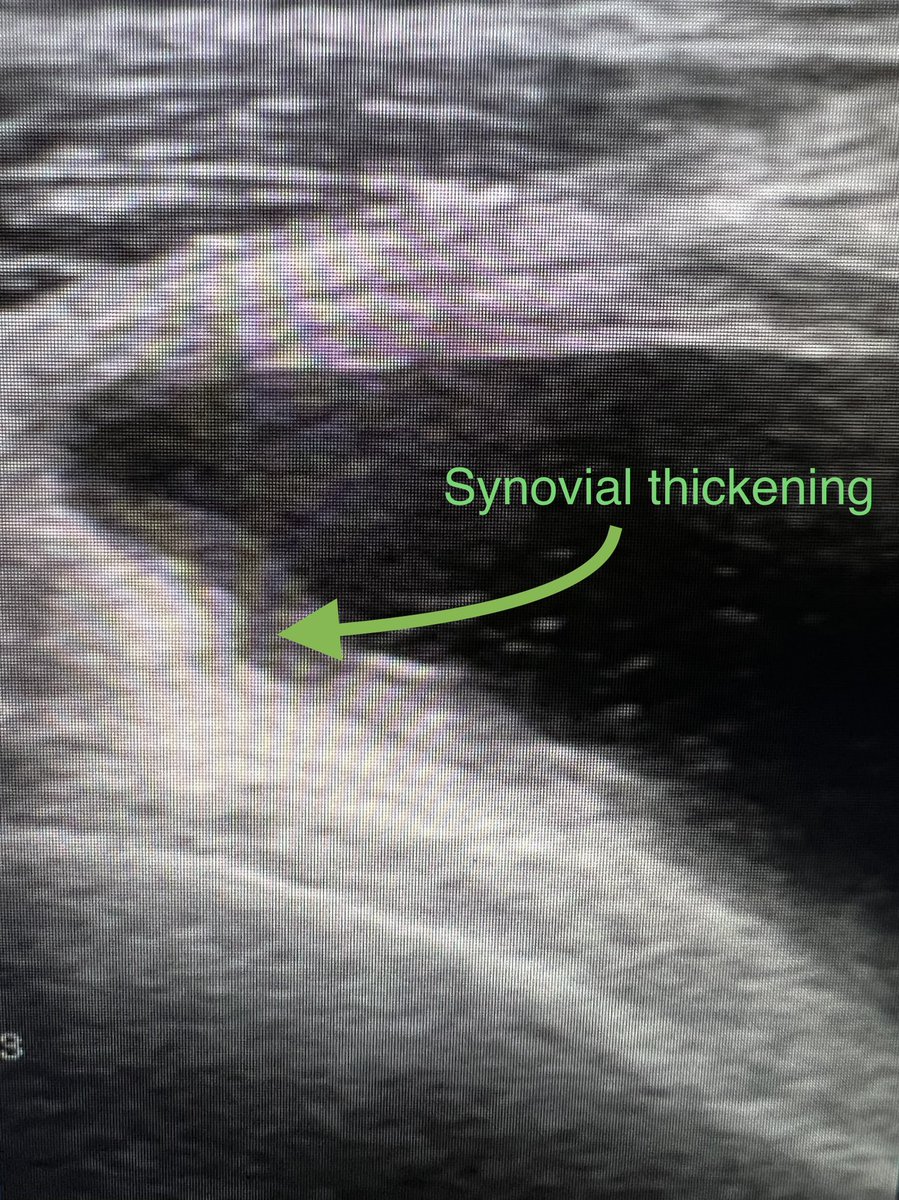
Useful to look closely at the synovium of the suprapatella pouch when scanning a patient with a knee effusion. Thickened synovium often becomes clear against the black contrast of the fluid. Perhaps more sensitive than MRI?
This patient has seronegative inflammatory arthropathy.
Interested to know if anyone else has come across the subacromial bursa snapping underneath the conjoint tendon? Patient has flicking sensation ant shoulder/chest which presumed to be LHB but US shows otherwise. Seen this a few times now.
An “internal snapping” shoulder perhaps!
@Vilavaite How do we classify normal in terms of muscle condition/deconditioning? We describe fat atrophy of certain muscle groups eg rotator cuff but it’s always subjective. Thoughts welcome!
I think we should be commenting more on muscle conditioning on MRI.
This lady has bilateral trochanteric bursitis and obvious global gluteal muscle deconditioning (streaky muscles with fatty infiltrates!) For me, this is the more important finding above an inflamed bursa.