Fact check: False
The fatality rate on this viral tweet is way too high, as the calculation involves the IFR, not the CFR. The real numbers are bad enough. Let’s stick to those.
@jacksonstuart93 Ed Yong has been such a solid reporter during this whole pandemic. This type of article seems so different tonally from what he's been writing.
.@edyong209: “A country that, 7 months into a pandemic, still cannot ensure that its healthcare workers have enough gowns and gloves and protective equipment is not going to be able to distribute a vaccine in an efficient way. It simply isn’t.”
AS A STATISTICIAN, I respect science expertise because I need it to do my job right. In the early days of the pandemic, I saw debate develop between those advocating we listen to experts and those who felt we should listen to the data. This is a false dichotomy, let me say why...
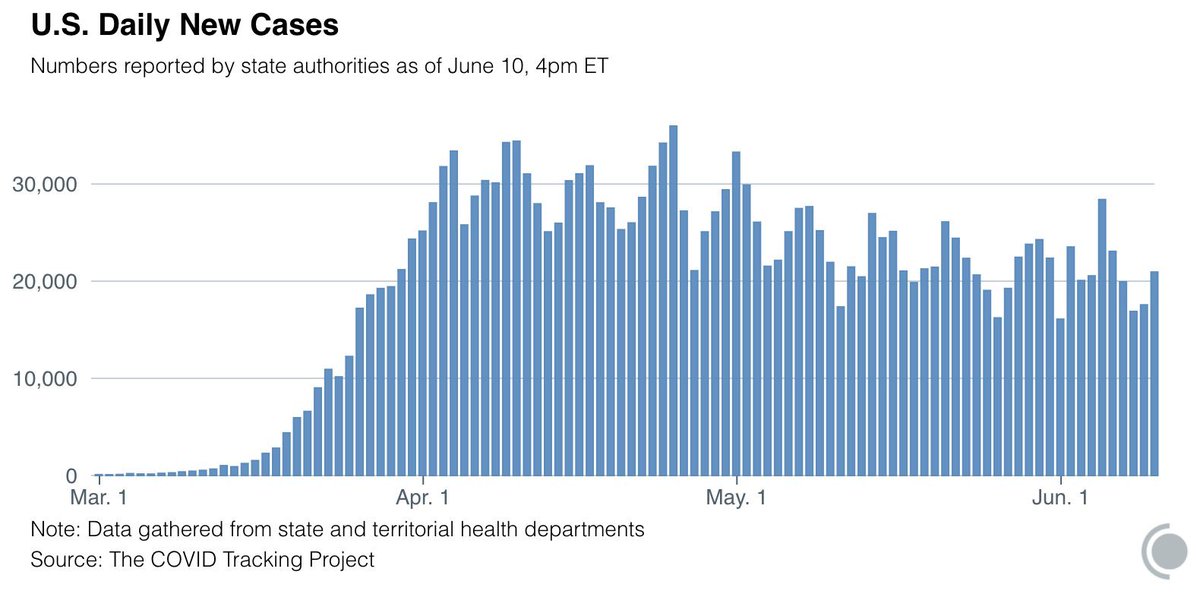
THINK LIKE AN EPIDEMIOLOGIST: why are COVID deaths *still* not going up 3 weeks after case counts started increasing? There are many possible explanations, but one I haven’t seen mentioned is the impact of widespread testing on *early detection*.
A #tweetorial on LEAD TIME BIAS.
The trillion dollar question. Why are COVID cases increasing while deaths are decreasing? The answer is simple. It's called Simpson's paradox and it's the result of incorrectly pooling data and arriving at a false conclusion. A thread 1/9 #COVID19#ThursdayThoughts
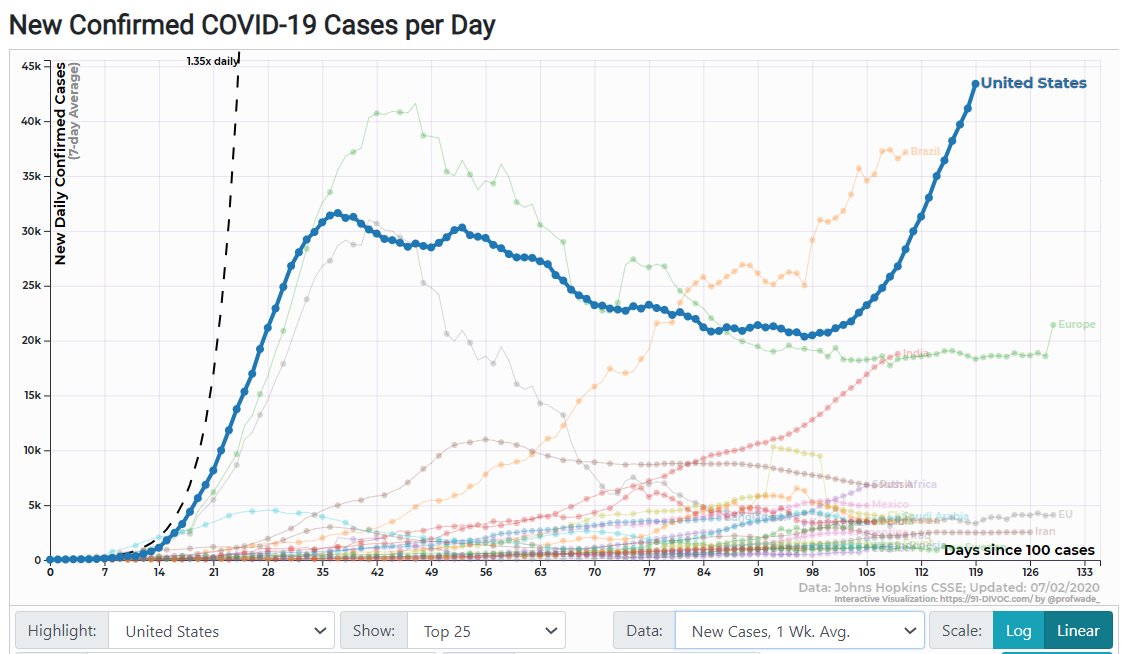
THINK LIKE AN EPIDEMIOLOGIST: There are more new confirmed cases each day in the US than at any time during the earlier April peak. But is it really meaningful to compare those numbers? How do epidemiologists decide when to sound the alarm? A thread. 1/11
I’ve seen plenty of zoos make statements about supporting BLM and diversity initiatives, but I’ve yet to see one announce that they’ve decided to abolish unpaid internships so that Black people without the generational wealth of their white peers can actually access zoo careers.
THINK LIKE AN EPIDEMIOLOGIST:
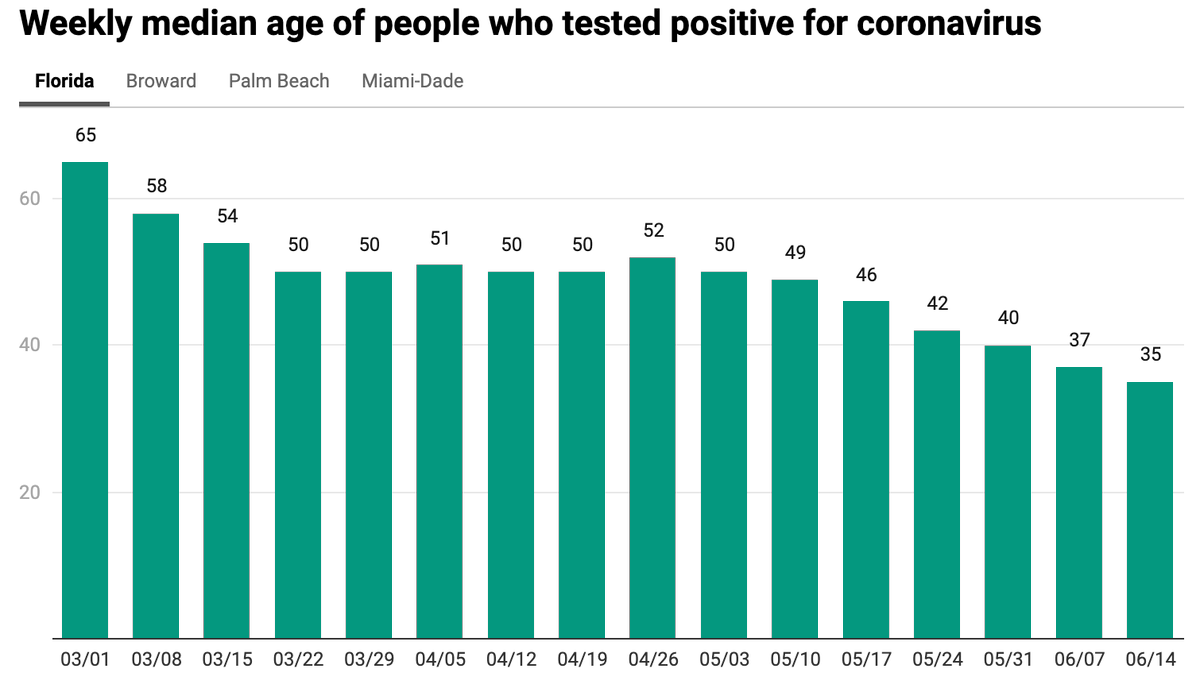
What does it mean that the median age of new cases is dropping in some areas? I see three possible explanations, not all good. A thread on how to distinguish between them. 1/10
(Figure h/t @ScottGottliebMD)
"When you do testing to that extent, you are going to find more people, you will find more cases. So I said slow the testing down."
—Trump on trying to keep the number of reported COVID cases low
Is everyone reading this??!
I gotta break down this science real quick.
This study compared COVID-19 mortality rates by racial/ethnic group AND age. It found:
Among folks aged 35-44, Black people had a COVID mortality rate 9 *times* as high as whites.
https://t.co/WJZINd6Rtt
Spoke with a biostatistician today who is deep in covid data and when they were asked if they're eating out on restaurant patios now, they literally laughed out loud.
BREAKING: The Trump administration just finalized a rule that would remove nondiscrimination protections for LGBTQ people in health care and health insurance.
Nationally there’s no “second wave.” There’s one long wave. We’ve been in a plateau of around 20,000 cases and 1,000 deaths a day, largely among minority and vulnerable populations. Reopening will cause spikes, but calling them a second wave denies the reality of what’s going on.
Three months ago, I paused book leave to return to the Atlantic for fulltime pandemic reporting. Here's a thread of 5 big pieces I've written since.
1) A sweeping look at how we got here, what must happen next, & the possible aftermath.
https://t.co/woc4dxfi9r
As a global public health expert, I don’t accept that US & UK poor responses were due to capacity. Poorer countries did much better. It’s down to absent leadership, incompetence & a deliberate decision to treat COVID-19 like flu for weeks in Feb & March & just ‘let it go’.
Saying "Race is a risk factor" is problematic. Statisticians and social scientists need to be more careful about this kind of language and avoid it where possible ...