Nephrologist FACP FASN | In love with Medicine | MKSAP-Reviewer Renal-physiology| EmoryNephrology | MorehouseMedicine | Love & hate Politics| Faith+Optimism🇺🇸
NEW on the #AJKDBlog:
@Maximal_Change interviews Manuel Laslandes and @c_massoumipour on response to rituximab as a maintenance therapy in adults with idiopathic nephrotic syndromes (INS):
https://t.co/Uzke8613fv
Association of Ertugliflozin on Kidney Outcomes in People After and Without an Interval Cardiovascular Event: Observations From the VERTIS CV Trial
https://t.co/yoLE3mDsFk (FREE)
Risks of Hypocalcemia and Other Bone Mineral Disorders for Denosumab Versus Zoledronate Across the Spectrum of Kidney Function: A Target Trial Emulation
https://t.co/T4zgAUgUUK
@jjcarrero1
An outstanding tribute to Helmut Rennke, a giant of renal pathology. @SethiRenalPath delivers the Helmut Rennke Endowed Lectureship on MPGN past, present, and future. A must-attend for all clinicians and pathologists.
#RenalPathology#MPGN#GlomConHawaii2026#Nephrology #ScientificExcellence
This was a difficult but good teaching case.
Easy to call idiopathic MPGN but…
LM: Membranoproliferative Glomerulonephritis (MPGN) pattern
IF- dull minimal IgG IgM C3 kappa lambda
EM- massive deposits.
Pronase IF/IgG subclass all negative. At this point I had an idea-
FIBRONECTIN GLOMERULOPATHY
Did mass spectrometry. Confirmed the diagnosis=Large amounts of fibronectin.
55 yr old with proteinuria and declining renal function.
In A Few Words essay by Adam Krieger:
"Dialysis keeps people alive, but it also consumes them. We cannot dialyze a broken system, and we must not allow that system to dialyze away our vigilance."
What We Cannot Dialyze https://t.co/nPZx5V9J8u (FREE)
@TulaneMedicine
Once again Last Month in Nephrology comes through. Great discussion about fluids in ICU sepsis (ARISE study 6/11 NEJM) . LESS may be more, clearly more in NOT more. Supports my statement that "volume is the new uremia". https://t.co/VuP84A5bgN
Advanced HF + hypotension creates a frustrating dilemma:
You need GDMT to improve outcomes.
You need blood pressure to give GDMT.
Does midodrine help with this or just add additional pharamcologic complications and noise?
This retrospective study <https://t.co/JyWNBAiE2V> found more GDMT initiation and uptitration with midodrine—but no improvement in survival and more hospitalizations 🤷🏻♂️
Overlap of C3GN and TMA (aHUS).
Both are complement-mediated diseases.
The study is the 1st to show overlap of C3GN-TMA findings in C3GN.
TMA findings are present on electron microscopy & maybe missed.
The lesions are often C3GN-dominant or TMA-dominant.
https://t.co/oZXxywGMKm
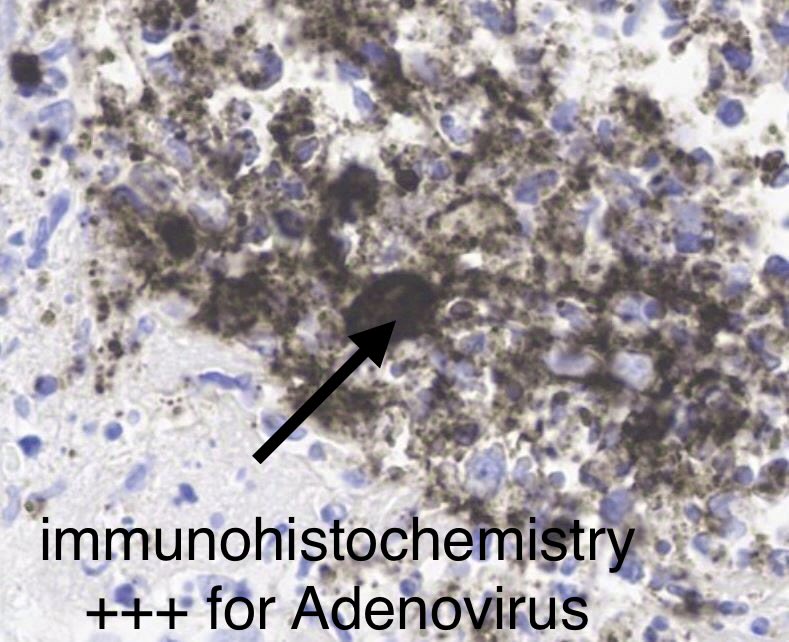
Kidney biopsy: Great teaching case
Severe inflammation and necrosis with abscess formation.
Look carefully=you see cells with large nuclei in the mix of inflammatory cells.
IHC= Positive staining for ADENOVIRUS.
DX: Adenovirus-associated interstitial nephritis.
55-yr old with kidney &
heart transplant, fevers, rise in serum creatinine.
I love this study but it is easy to take the lessons too far. All of the 49,000 biopsies only happened after a nephrologist thought, "This doesn't look like DKD, we should get a biopsy"
What is the approach to polyclonal hypergammaglobulinemia?
What is the differential diagnosis for a patient with tubulointerstitial nephritis and polyclonal hypergammaglobulinemia?
Quiz: https://t.co/2loGM0S52a (FREE)