In cases showing diffuse bronchiectasis related to infection (not traction bronchiectasis, which is a feature of fibrotic lung disease), it is important to remember that bronchiectasis itself is not a diagnosis. It reflects an underlying cause, and the radiologist should try to suggest that cause based on the pattern and distribution.
A practical first step is to assess whether the diffuse bronchiectasis is central or peripheral.
•Central bronchiectasis has a limited differential.
•With upper lobe predominance, consider cystic fibrosis and allergic bronchopulmonary aspergillosis.
•With lower lobe predominance, consider primary ciliary dyskinesia and immunodeficiency.
•Peripheral bronchiectasis also provides clues.
•Predominance in the right middle lobe and lingula suggests Mycobacterium avium complex infection.
•Lower lobe–predominant peripheral bronchiectasis may point toward rheumatoid arthritis–related airway disease.
Across these entities, diffuse bronchiectasis is often accompanied by tree-in-bud nodules and mucus plugging, reflecting active or recurrent infection.
👉 Based on these basic imaging principles and the provided videos, what is your diagnosis or differential diagnosis in this case?
🎯Increasing the CT attenuation threshold to 20 HU for lesions < 4 cm and eliminating washout CT for true adrenal incidentalomas, together with recommendations for endocrine assessment, will significantly decrease the over-investigation of overwhelmingly benign adrenal lesions.
Here’s how to make hippocampal anatomy memorable!
This video shows hippocampal anatomy that you need to stay in your hippocampus!
--Body is where you can see the spiraling line that is the Cornu Ammonis.
--Cornu Ammonis spirals into the dentate nucleus so that they look like a yin-yang.
The theme of hippocampal anatomy is the spiral—on every single hippocampal MRI, you should look for that T2 dark line of the Cornu Ammonis or SLRM, spiraling into the dentate to make a yin yang!
If this is lost, that is an early sign of MTS.
This month’s @rsnagram @Radiographics has all you need to know about epilepsy, how we image it & how we treat it!
Check it out: https://t.co/QEyDPx1zMD
So now you know the basics of hippocampal anatomy—may you never forget the hippocampal spiral!
@cookyscan1@radiographics@RadG_Editor
In this VideoGIE article, Diego Cadena Aguirre et al examine "Buried lumen-apposing metal stent following EUS-guided gastrojejunostomy: a rare adverse event and its management." https://t.co/CA0wStayad
@DiegoCadenaA@KaraRaphael
Señor Director del IESS @EdgarLamaVonB ,
¿Cómo es posible que después de dos días pidiendo atención médica urgente, recién hoy se haya subido a un paciente con hemorragia cerebral a la Unidad de Cuidados Intensivos (UCI)?
🧵 Abro Hilo (por favor RT🙏)
#URGENTE#DialogandoEntrePanas ⭕ informa:
➡️ Ayúdanos a Encontrarlo | Pedro Gustavo Merino Benavides, fue visto por última vez el 4 de marzo de 2025 en el sector de La Granados, #Quito.
➡️ Si tienes información llama al 1800-DELITO
La periodista quiteña @janethinostroza ha compartido un mensaje importante para los ecuatorianos, repasando la historia del país y destacando los eventos más importantes de los últimos 61 años. En su mensaje, explica cómo llegamos a la situación actual y propone acciones para mantener el orden y la democracia en Ecuador. Aunque algunos puedan interpretarlo como un apoyo al gobierno, su mensaje busca que el Ecuador se convierta en un país de ‘verdad’. No de mentiras.
El comentario de @jxbenedeti en #PuntoDeOrden ⤵️
https://t.co/PhShiT0xVI
#Testimonios | Hay enfermos con males catastróficos que no recibieron sus medicinas, incluso a pesar de que la justicia ecuatoriana ordenó la entrega de tratamientos. https://t.co/IN6VHhTvPl
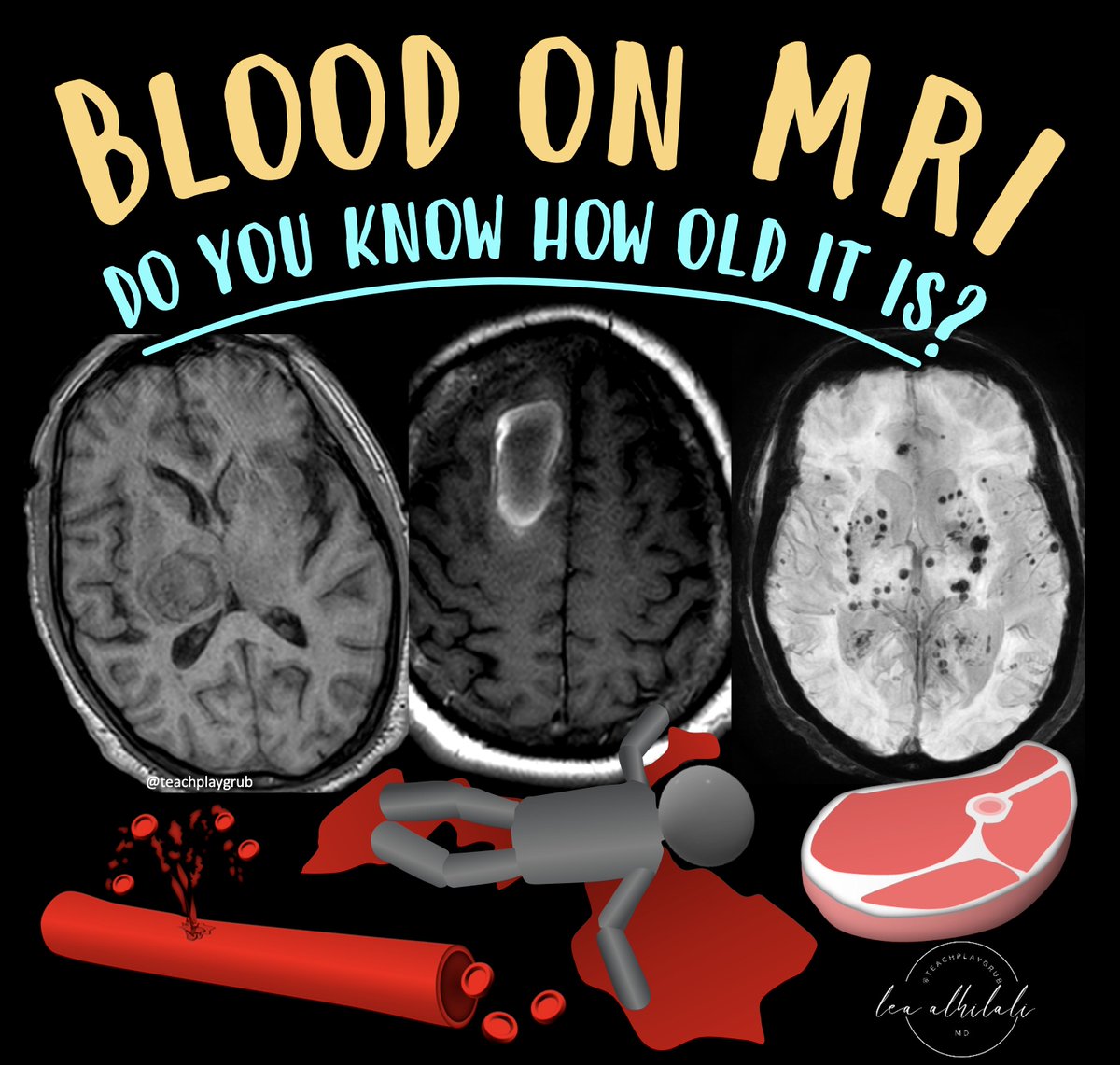
1/Asking “How old are you?” can be dicey—both in real life & on MRI! Do you know how to tell the age of blood on MRI?
Here’s a thread on how to date blood on MRI so that the next time you see a hemorrhage, your guess on when it happened will always be in the right vein!
🤖 ¡Hola a todos! vamos a desglosar el artículo "Criterios Diagnósticos para la Fibrosis Pulmonar Idiopática" publicado en @TheLancet. ¿Sabías que la TC puede diagnosticar FPI sin biopsia en algunos casos? ¡Hilo con todos los detalles!🧵 #FOAMrad#MedEd@residentesSERAM
La familia y compañeros de Edwin Ortiz, del Cuerpo de Bomberos de Zamora, realizan una colecta para cubrir los gastos médicos. Conozca cómo apoyar al bombero. https://t.co/A7XCaHt6yT
¡Te recibimos con los brazos abiertos Lisseth Ayoví!🇪🇨
La halterista ecuatoriana ya se encuentra en Ecuador, tras su gran debut en los Juegos Olímpicos París 2024.
#Opinión ✍ | "El buen momento por el que atraviesa el deporte nacional, por fuera del fútbol, (...) hace sacar tres lecciones que estos gladiadores olímpicos son capaces de dar a la política".
Revisa el newsletter #CódigoRojas y suscríbete 📲 https://t.co/rXLWGANjnj
Can the MRI findings of a meniscal tear tell us if its treatment should be surgical?
According to multiple studies, magnetic resonance imaging is an excellent tool to confirm the presence of a meniscal tear, with a sensitivity and specificity of around 96-97%. Furthermore, it has high precision in suggesting the type of tear and thus can determine if it is a stable or unstable injury, extrapolating the arthroscopic criteria described.
However, the indication for surgical treatment should be based on clinical findings and after the failure of less invasive medical treatments, with joint block probably being the only indication for immediate surgery.
Three cases of meniscal tears considered unstable by arthroscopic criteria that did not require surgical treatment are presented.
In the first example, a bucket-handle tear of the medial meniscus is seen in a patient with an MRI requested for suspected patellar tendinopathy. As it is a radiological finding, the athlete who reported self-limited medial pain two years before this MRI was re-interviewed. We have followed up for 13 years without joint blockage, effusion, or concomitant alterations in imaging studies.
In the second case, a complete radial tear was seen at the junction of the body with the anterior horn of the external meniscus, with involvement of the meniscal wall, which was treated with anti-inflammatory physiotherapy techniques associated with parameniscal infiltration with corticosteroids guided by ultrasound and accompanied by management of the biomechanical origin at the level of the iliotibial band, with complete resolution of symptoms in 15 days and return to sports activity after 24 days, with a 4-year MRI follow-up without chondral, meniscal or bone alterations.
In the last study, there was a flap tear in the posterior horn of the internal meniscus in a patient in whom the examination was performed for a sports checkup, with clinical and radiological follow-up for six years without subsequent alterations.
Thanks to Dr.Sherelle Laifer-Narin yesterday for the wonderful lecture on Placental abnormalities at the SABI monthly webinar series! @SABImaging
If you missed it, SABI members are free to see it on https://t.co/ygRHHuGN0Q soon! Stay tuned!
@ASBEpic @ivpedrosa