💊 Digoxin Dosing Made Simple:
✅ IV loading dose.
✅ Maintenance dosing.
✅ Dose adjustment.
✅ Essential monitoring.
✅ Toxicity pearls.
Save it for your next cardiology rotation and share with a colleague who needs it.
#MedTwitter#FOAMed#Cardiology#Medicine
🩺 Approach to Acute Kidney Injury (AKI)
AKI is a medical emergency—recognize it early, identify the cause, and intervene before irreversible kidney damage occurs.
AKI is defined by a rapid decline in kidney function, resulting in rising serum creatinine and/or reduced urine output. The key to management is determining whether the cause is pre-renal, intrinsic renal, or post-renal.
📚 Stepwise Approach to AKI:
1️⃣ Think AKI
• Rising creatinine or oliguria (<0.5 mL/kg/hr).
• Review previous renal function and identify high-risk patients.
2️⃣ Confirm the Diagnosis
• Repeat renal profile.
• Perform urinalysis and monitor urine output.
• Review medications, recent contrast exposure, and comorbidities.
3️⃣ Classify the Cause
🟢 Pre-renal: Hypovolemia, sepsis, heart failure, cirrhosis.
🔵 Intrinsic: ATN, glomerulonephritis, AIN, vasculitis.
🟠 Post-renal: Urinary tract obstruction (BPH, stones, malignancy).
4️⃣ Investigate Systematically
• Assess volume status and blood pressure.
• U&Es, bicarbonate, urinalysis, urine sodium/osmolality.
• Renal ultrasound if obstruction is suspected.
5️⃣ Treat the Underlying Cause
✔️ Restore perfusion in pre-renal AKI.
✔️ Stop nephrotoxic drugs (NSAIDs, ACEi/ARB where appropriate).
✔️ Relieve urinary obstruction promptly.
✔️ Correct electrolyte abnormalities and monitor fluid balance closely.
💡 High-Yield Exam Pearls
✔️ ATN is the most common intrinsic cause of AKI.
✔️ Always exclude post-renal obstruction with renal ultrasound.
✔️ Hyperkalaemia, severe metabolic acidosis, pulmonary oedema, and uraemic complications require urgent nephrology review and consideration of dialysis.
✔️ Treat the cause, not just the creatinine.
📖 Want more concise, exam-focused nephrology notes?
Visit https://t.co/2UQyCbb6in and explore our Nephrology & Urology book—designed for medical students, MRCP, USMLE, PLAB, AMC, and everyday clinical practice.
❤️ Save this post for revision.
📤 Share it with your colleagues.
💬 What investigation do you always order first when assessing AKI?
#AKI #AcuteKidneyInjury #Nephrology #InternalMedicine #MedicalStudent
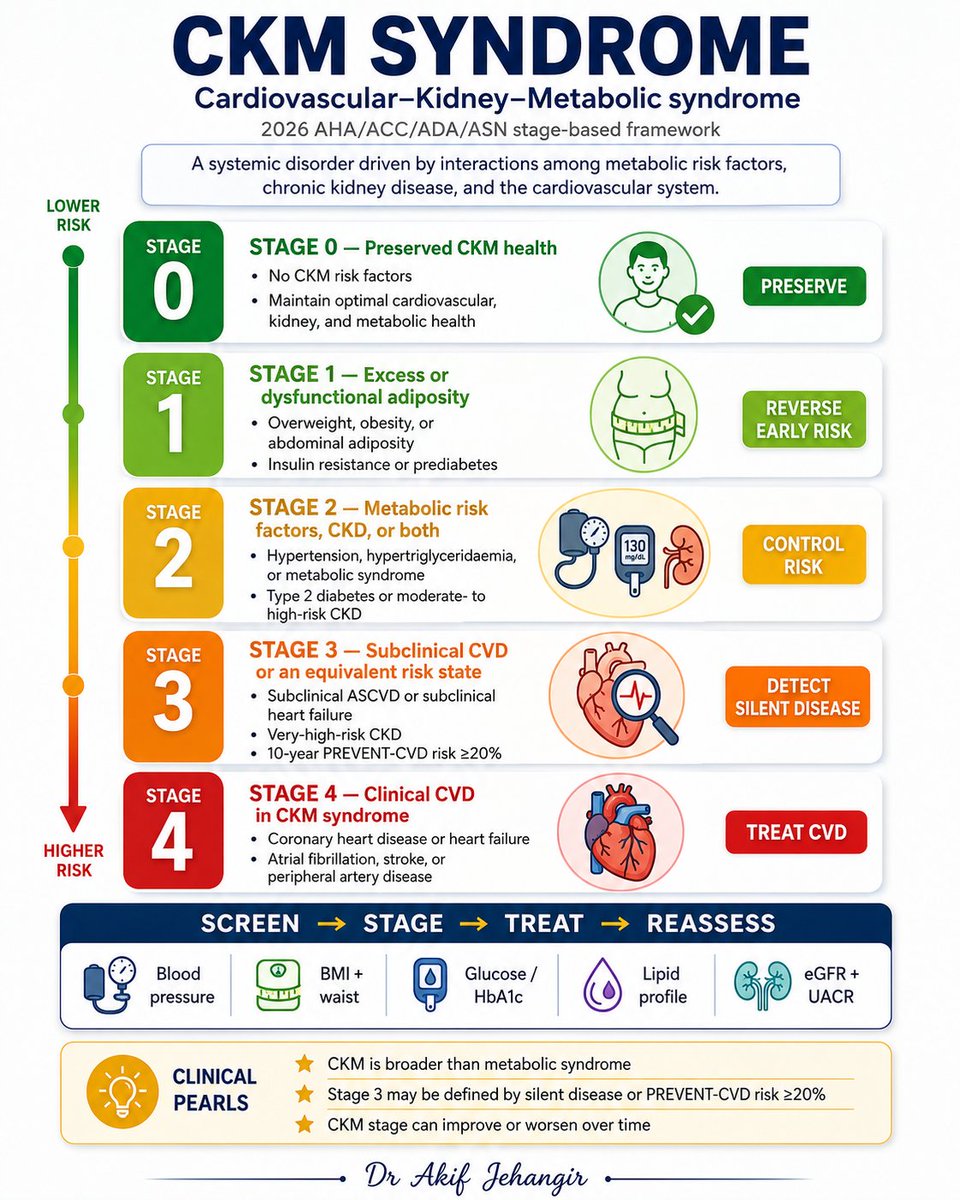
Cardiovascular–kidney–metabolic syndrome links obesity, diabetes, chronic kidney disease, and cardiovascular disease into one connected framework. Understanding the stage helps you screen earlier, stratify risk better, and intervene before overt cardiovascular events develop
💧 7 Causes of Hyponatremia
Low sodium is a finding—not the diagnosis. The key is identifying the underlying mechanism.
Hyponatremia (serum Na⁺ <135 mmol/L) is one of the most common electrolyte disorders encountered in clinical practice. A systematic approach using serum osmolality, volume status, and urine studies helps narrow the differential diagnosis.
📚 7 High-Yield Causes:
1️⃣ Primary Polydipsia (Excess Water Intake)
• Excess free water overwhelms renal excretion.
• Low urine osmolality and dilute urine.
2️⃣ SIADH
• Excess ADH → water retention without oedema.
• Euvolemic hyponatremia with high urine osmolality and high urine sodium.
3️⃣ Thiazide Diuretics
• Common drug-induced cause, especially in elderly patients.
• Causes renal sodium loss with impaired urinary dilution.
4️⃣ Hypovolemic Hyponatremia
• Sodium loss exceeds water loss.
• Seen with vomiting, diarrhoea, adrenal insufficiency, or diuretics.
5️⃣ Hypervolemic Hyponatremia
• Total body water and sodium increase, but water retention predominates.
• Common in heart failure, cirrhosis, nephrotic syndrome, and advanced CKD.
6️⃣ Adrenal Insufficiency
• Cortisol deficiency increases ADH secretion.
• Think of hyponatremia with hypotension, hyperkalaemia, weight loss, or hypoglycaemia.
7️⃣ Hypothyroidism
• Reduced cardiac output and GFR impair free water clearance.
• Usually causes mild chronic hyponatremia.
💡 Exam Pearls
✔️ Always classify hyponatremia as hypovolemic, euvolemic, or hypervolemic.
✔️ Exclude adrenal insufficiency and hypothyroidism before diagnosing SIADH.
✔️ Severe symptomatic hyponatremia requires 3% hypertonic saline.
✔️ Chronic hyponatremia must be corrected slowly to prevent osmotic demyelination syndrome (ODS).
📖 Want more concise, exam-focused notes like this?
Visit https://t.co/2UQyCbb6in and explore our high-yield Nephrology & Urology book, designed for medical students, MRCP, USMLE, PLAB, AMC, and clinical practice.
❤️ Save this post for revision.
📤 Share it with your colleagues.
💬 Which cause of hyponatremia do you find hardest to remember?
#Hyponatremia #Nephrology #InternalMedicine #Electrolytes #MedicalStudent
Lupus and Hydralazine.
*A patient who develops lupus after prolonged hydralazine therapy is most likely to test positive for anti-histone antibodies.
*While antinuclear antibodies (ANA) will also be positive in almost all cases, anti-histone antibodies are the specific classic marker for Drug-Induced Lupus Erythematosus (DILE).
1. Understanding Drug-Induced Lupus (DILE).
DILE is a side effect caused by certain long-term medications
*High-Risk Triggers:
Hydralazine (used for high blood pressure) and procainamide (used for heart rhythm issues) are the most common causes.
*The Culprit:
Over 95% of patients with hydralazine-induced lupus develop anti-histone antibodies.
*The Difference:
Unlike regular (idiopathic) lupus, markers like anti-dsDNA and anti-Smith (anti-Sm) are usually negative here.
2. Genetic Risk Factor:
*Slow Acetylators.
The liver breaks down hydralazine using a process called acetylation.
Some people are genetically slow acetylators.
They process the medication much slower than normal.
This causes the drug to build up in the body, greatly increasing the risk of triggering the autoimmune reaction.
●Key Laboratory Differences
https://t.co/BcIH5iJoAu