Routine doesn't mean risk-free. When should you place an IVC filter, how do you place it optimally, and when should you take it back out?
In our latest episode, Dr. Daniel O'Neal joins guest host Dr. Jessica Yoon to step through the ins and outs of IVC filter placement and share his tips for long-term technical and clinical success.
🎧 Tune in on the BackTable app: https://t.co/Lutc3uMRO9
#VI650 #InterventionalRadiology #VIR #MedicalEducation #IVCFilter #FilterOut #DVT #PulmonaryEmbolism
This “How I Do It” video briefly describes a carotid body tumor case and provides narrated footage demonstrating how our vascular surgeons approach carotid body tumors.
👉 Continue watching this video, along with hours of other educational content: https://t.co/R2Q1wpg7EV. #VascSurg
🧵 Supraclavicular Decompression for Neurogenic Thoracic Outlet Syndrome — Anatomy, Technique & Pitfalls
Based on Thompson & Ohman (Washington University) "How I Do It" + Wind GG anatomy text + peer-reviewed literature
📺 https://t.co/U4ch1mEmm3
@westleyohman
🧵 Thread 👇
Carotid webs don’t cause stroke because of stenosis. The narrowing is minimal.
The problem is flow.
In this video, I walk through a DSA of a carotid web. You’ll see contrast accelerate over the web and then pool behind it. That pocket of stasis is exactly where clot forms.
Stasis alone satisfies Virchow’s triad. But stasis also kills shear stress, and the endothelial glycocalyx depends on shear to stay intact. When it thins, you lose its natural anti-clot functions, platelet inhibition, antithrombin III activation, and even local tPA support.
Stasis plus loss of glycocalyx creates the perfect setup for thrombus.
Watch the clip. Then check my previous post below for a deeper breakdown of carotid webs.
#Neurology #Neuroradiology #Stroke
🩻Contrast-induced AKI:
one of the biggest myths still shaping clinical decisions
For decades we were taught:
👉 “Contrast damages the kidneys”
👉 “Avoid CT with contrast in CKD”
👉 “Hydrate, protect, delay imaging if needed”
But what if… most of this is wrong?🤔
->The uncomfortable reality
Modern evidence shows:
👉 Low-osmolar contrast rarely causes true nephrotoxicity
👉 Even in CKD, AKI, and ICU patients
👉 The risk is often overestimated—or nonexistent
So where did the fear come from?
📍 1950s high-osmolar contrast (actually toxic)
📍 Poorly controlled observational studies
📍 “Creatinine rise = contrast injury” assumption
👉 Correlation became causation
👉 And the dogma stayed
⚠️What recent data tells us
✔ No difference in AKI rates with vs without contrast
✔ No benefit from bicarbonate, NAC, or aggressive hydration
✔ Even ICU and AKI patients show no worsening outcomes
->Translation to real life
👉 The patient was going to develop AKI anyway...Not because of contrast!!
->The real problem: “Renalism”
👉 Avoiding necessary imaging
👉 Delaying diagnosis
👉 Choosing inferior tests
And that leads to:
❌ Missed PE
❌ Delayed sepsis source control
❌ Worse outcomes
->Clinical mindset shift
Instead of asking:
👉 “Will contrast harm the kidneys?”
We should ask:
👉 “Will NOT doing the scan harm the patient?”
->Who still deserves caution?
✔ eGFR <30
✔ Severe hemodynamic instability
✔ Multiple nephrotoxins
Even then:
👉 Optimize volume
👉 Minimize dose
👉 Don’t delay critical imaging
🤓Bottom line
✔ Contrast nephrotoxicity exists… but is rare
✔ The fear is bigger than the risk
✔ The harm of NOT imaging is often greater
In critical care
👉 We don’t treat creatinine
👉 We treat patients
And sometimes…
👉 The most dangerous thing is NOT the contrast
👉 It’s hesitation.
📃Reference
Florens N, Demiselle J.
Kidney360 7: 445–449, 2026. doi: https://t.co/CWzi7WC9Wx
🧵 NEW STUDY: Eversion CEA vs. Conventional CEA with patch angioplasty. 180,000 patients, 13 years of data from the VQI database. Which technique wins? Let's break it down 👇 1/7
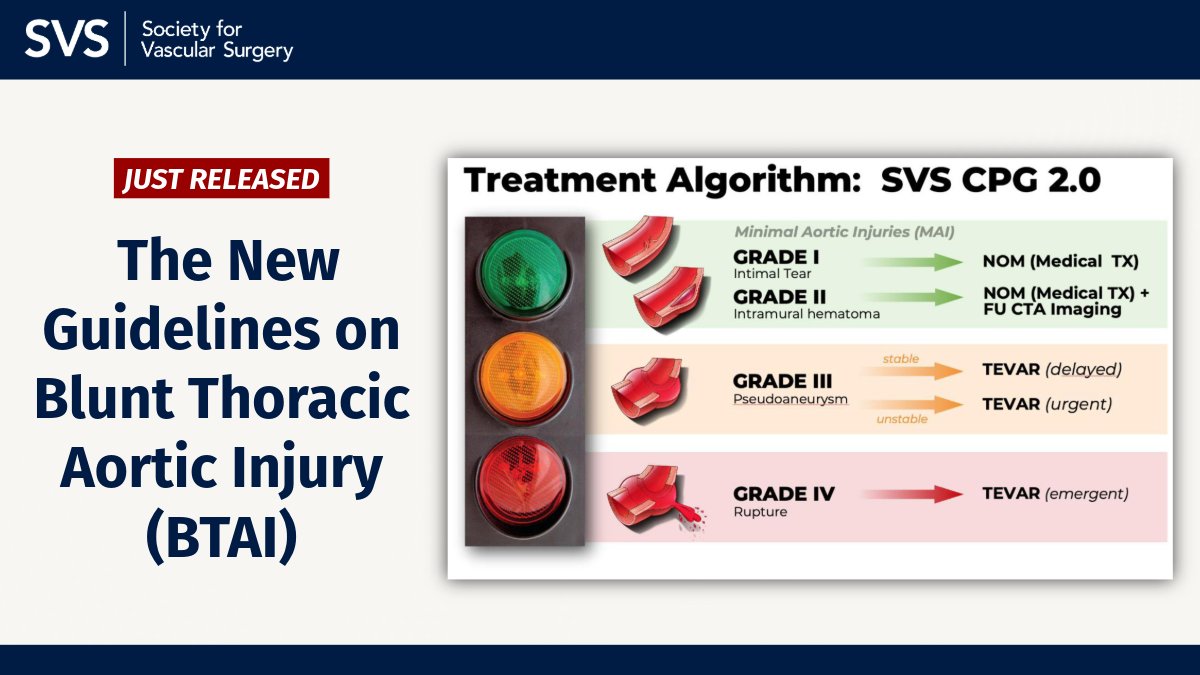
The new guidelines on the management of Blunt Thoracic Aortic Injury (BTAI) are out!
This release includes 13 updated recommendations based on more than a decade of new research.
Learn more: https://t.co/Gb3NudNIxw
#VascSurg#BTAI#Quality#Guidelines
ATLS 11th Edition.
https://t.co/NTVVcqrGbP
A significant update in the 11th Edition of Advanced Trauma Life Support introduces the xABCDE algorithm, prioritizing control of exsanguinating external hemorrhage before proceeding to airway management.
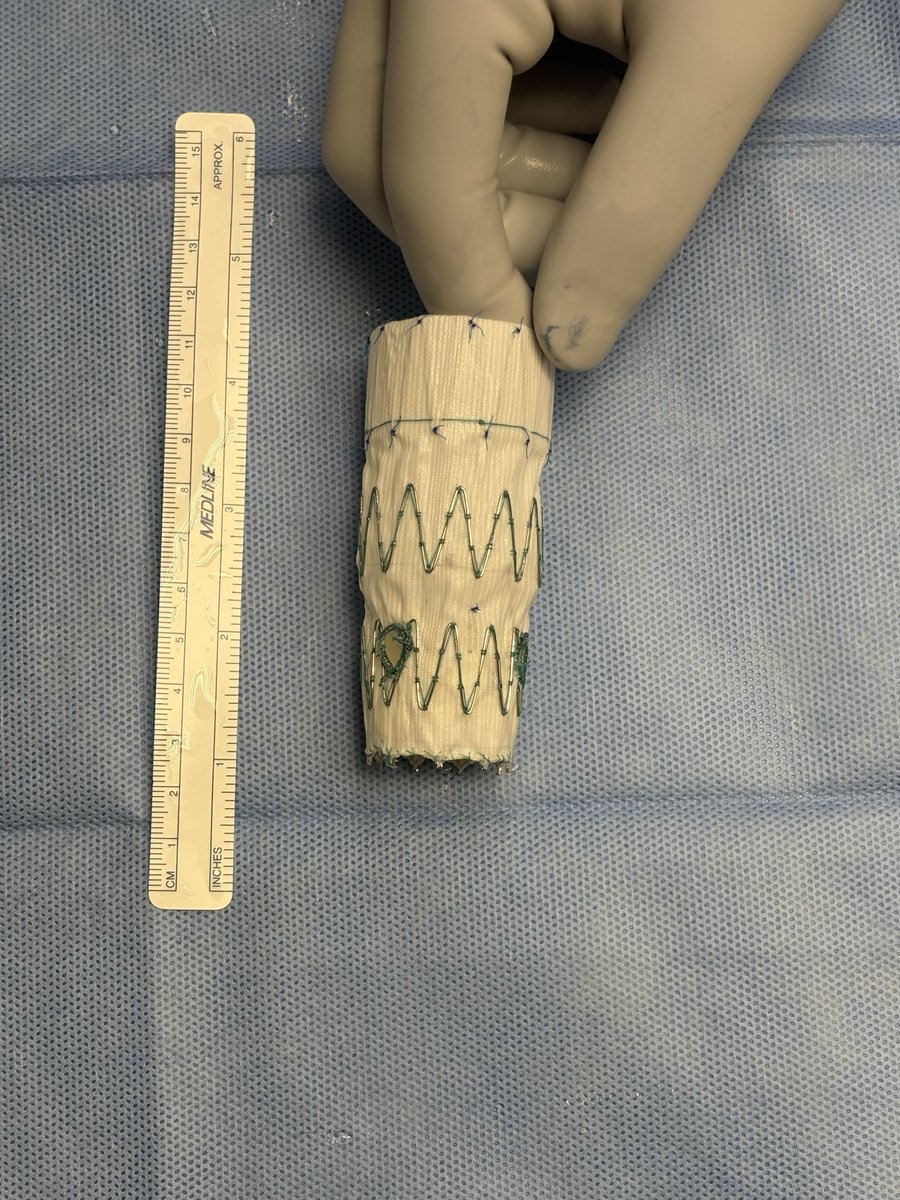
Gore recently announced the first implantation of the investigational Gore ascending stent graft in the ARISE III trial for the treatment of an acute type A dissection @WLGore https://t.co/qWdvKIOcbh
The 11th Endo-Bentall + arch PETTICOAT Technique was successfully performed at UM for an acute type A aortic dissection. Kudos to the entire team, especially Dr. Shah and Dr. Gupta. The patient was discharged home a few days later with no complications.@dr_ghoreishi @UMMC @MarylandVasc
Fantastic how-to VASCULAR SHUNT🩸 video from @NatalieADrucker@bryanacotton1@UTHealthACS 👇🏼👇🏼👇🏼
Find more high-quality trauma videos ➡️➡️ https://t.co/BxATsMqHPY
+++ Trauma Surgery Video Atlas ➡️ https://t.co/YimZHUcAwB
A carotid web (CaW)—also called a carotid diaphragm—is thought to be an intimal variant of fibromuscular dysplasia (FMD).
It appears as a thin, shelf-like projection of the tunica intima arising from the posterior wall of the ICA, just distal to the carotid bifurcation, and projecting anteriorly into the lumen.
The size and angle of the projection differ from patient to patient—but the larger the web (≥3 mm) and the more vertically oriented it is (more acute angle relative to the carotid wall), the greater the risk of stroke.
CaWs are more common in women and in African American patients.
When to suspect a carotid web?
Most ischemic strokes come from aging vessels and hearts: atherosclerosis, small-vessel disease, or cardioembolism from structural or functional cardiac disease.
But in young patients (<40) without traditional vascular risk factors who present with a large cortical stroke, you must consider alternative mechanisms—including carotid web.
Classic setup:
A young, otherwise healthy patient → sudden large-vessel stroke → CTA “read as normal” unless the carotid bulb is carefully inspected.
How do we detect it?
In routine practice, CTA is the most common noninvasive test of the cervicocerebral vasculature.
CTA has excellent spatial resolution, allowing a trained eye to spot the characteristic shelf-like projection at the posterior carotid bulb.
I posted a CTA of a carotid web in the previous case (linked below). 👇👇
Can you see the shelf-like protrusion from the posterior wall? Click through to the prior post and train your eye to recognize this pathology.
Over the next day or so, I’ll post a short voice-over video explaining why this seemingly small shelf leads to embolic strokes. A video will do more than a long text explanation.
In the meantime:
Who can thoroughly explain why a carotid web is such an efficient generator of embolic stroke?
Reference
Chen H, Colasurdo M, Costa M, Nossek E, Kan P. Carotid webs: a review of pathophysiology, diagnostic findings, and treatment options. J Neurointerv Surg. 2024;16(12):1294–1299. doi:10.1136/jnis-2023-021243.
#Stroke #Neurology #Neuroradiology #FOAMed
I focus on DeBakey not only for his contributions to cardiac surgery, but his humanistic qualities to which we should aspire
“Real success requires respect for and faithfulness for the highest human values- honesty, integrity self-discipline, dignity, compassion, humility, courage, personal responsibility, courtesy, and human service” Michael DeBakey
Opinion of a vascular surgeon who is enthusiast of both stenting and or cea. Two points: why the divergence at 3-4 years? A flat lien for the stent group with simply no events over 1 year? The lack of significance between cea v medical therapy despite substantial gap - type 2 err underpowered for this late difference? Never forget: some anatomical lesion and arterial characteristics are simply not favorable for stents.
ANZAST Trauma Grand Rounds. Tuesday 2 December 2025 at 6:00 pm AEDT / 8:00 pm NZDT. "Trauma Surgery in Rural/Regional Australasia" and will be presented by Dr Tom Bowles with panelists Dr Merwe Hartslief and Dr Jacques Marnewick. Register: https://t.co/kHHIFvYsFQ
REBOA = higher mortality (47% vs 36%), more transfusions, longer time to OR. No survival benefit. Check the new study by Hatchimonji et al. https://t.co/RnQGoCdJXI and Jansen's commentary https://t.co/s3qqRcWi6C.
@jhatchmd @dianehaddadmd@pdowzicky@markseamonmd