Biallelic TP53 loss is NOT included in IMS/IMWG 2024 risk stratification.
Yet most would agree: this is ULTRA –High RISK myeloma.
WHY ? Because we only include what we can measure.
FISH detects del(17p) → only one hit
NGS detects mutation → may suggest double hit but misses many
VAF >60% is suggestive, not confirmatory
CMA/SNP is key:
• Detects copy-neutral LOH
• Mutant allele duplicates, wild-type lost
• True biallelic inactivation
We measure deletions… BUT biology operates through loss of function.
Bottom line:
FISH + NGS + CMA are needed for full TP53 assessment
Until then, we are under-calling ultra–high risk myeloma.
#myeloma #MultipleMyeloma #Hemetwitter #smmm
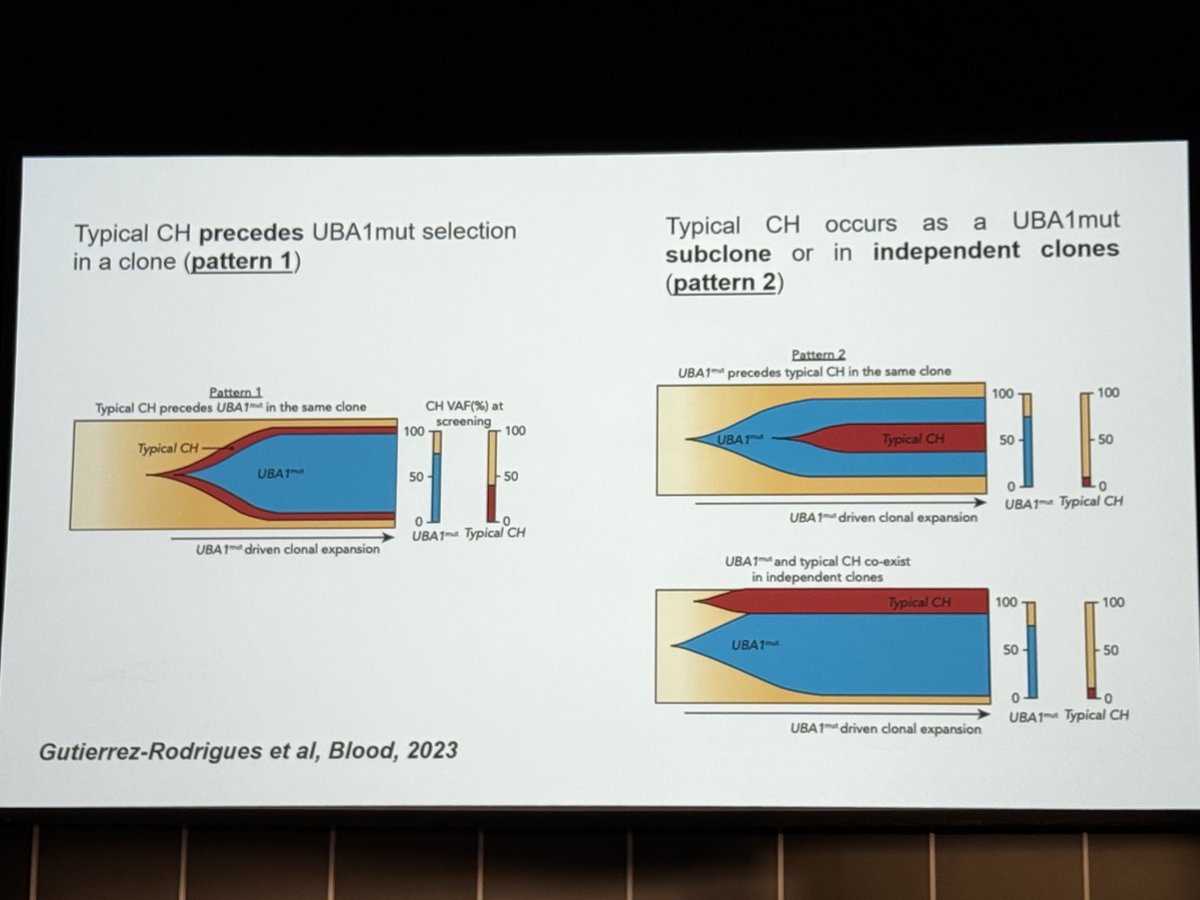
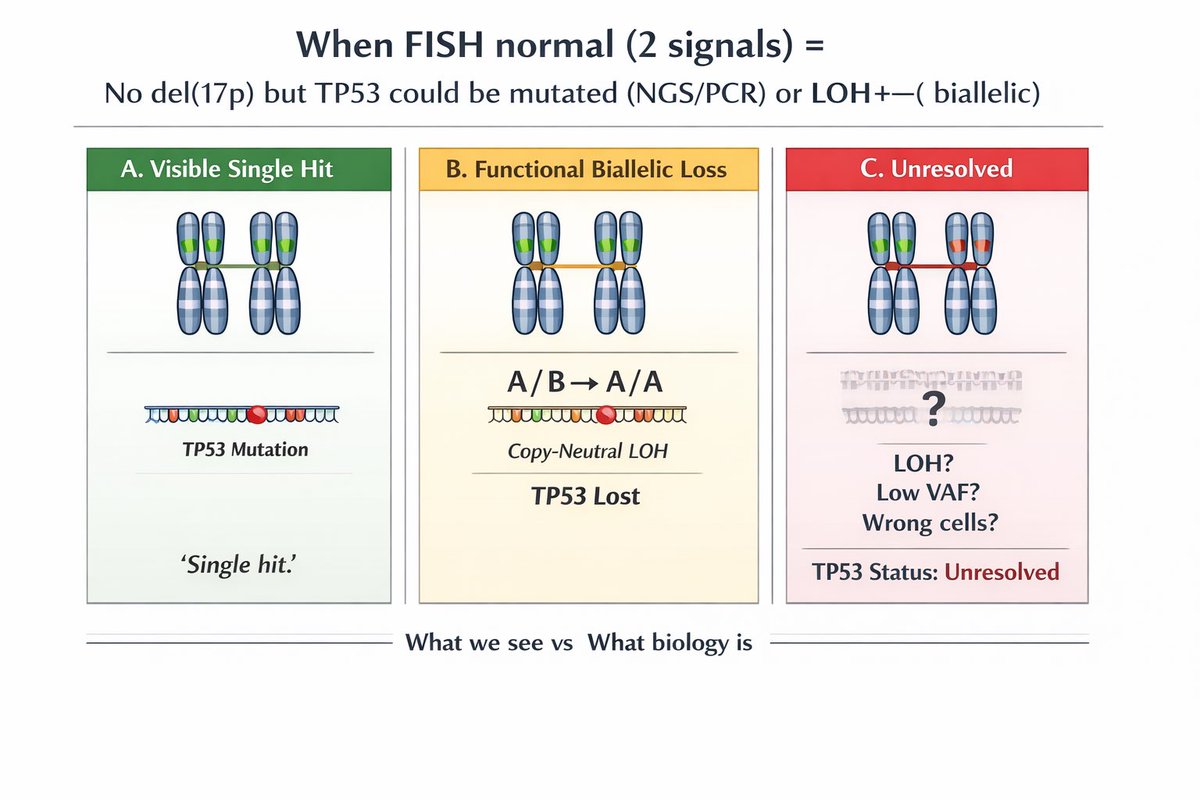
We said we are missing biallelic TP53.
Here is one reason why:
FISH “normal” (2 signals) ≠ intact TP53.
You can have:
• TP53 mutation (NGS/PCR)
• LOH → functional biallelic loss
• Or simply not tested / not detected
Not all “normal” results are equal.
What we see ≠ what biology is.
#smmm #myeloma #Medtwitter #Hemetwitter
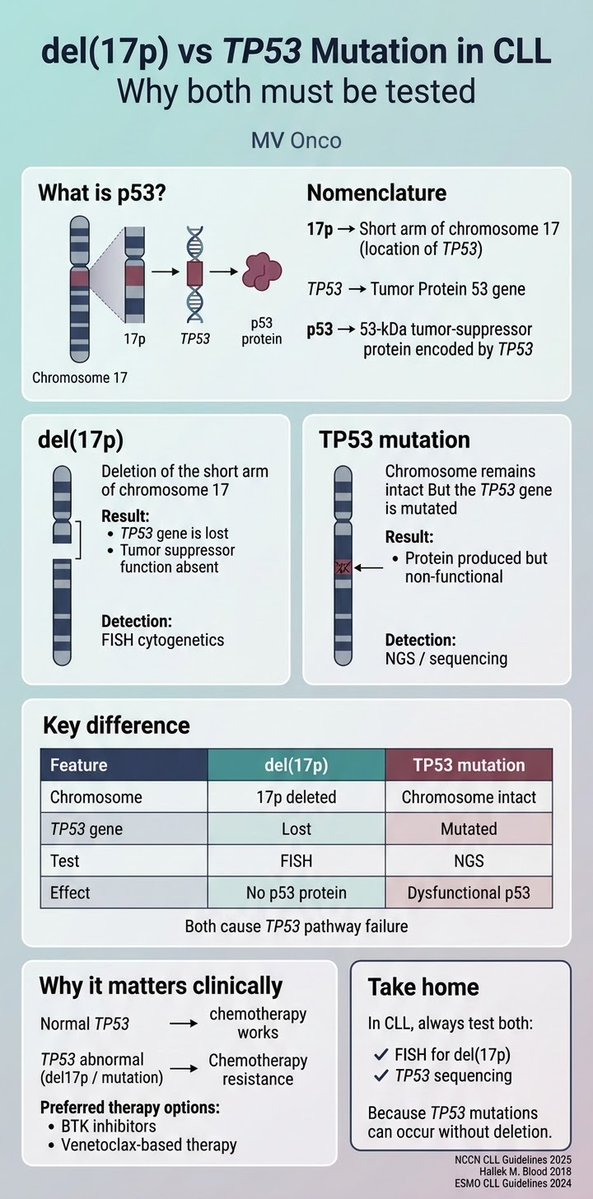
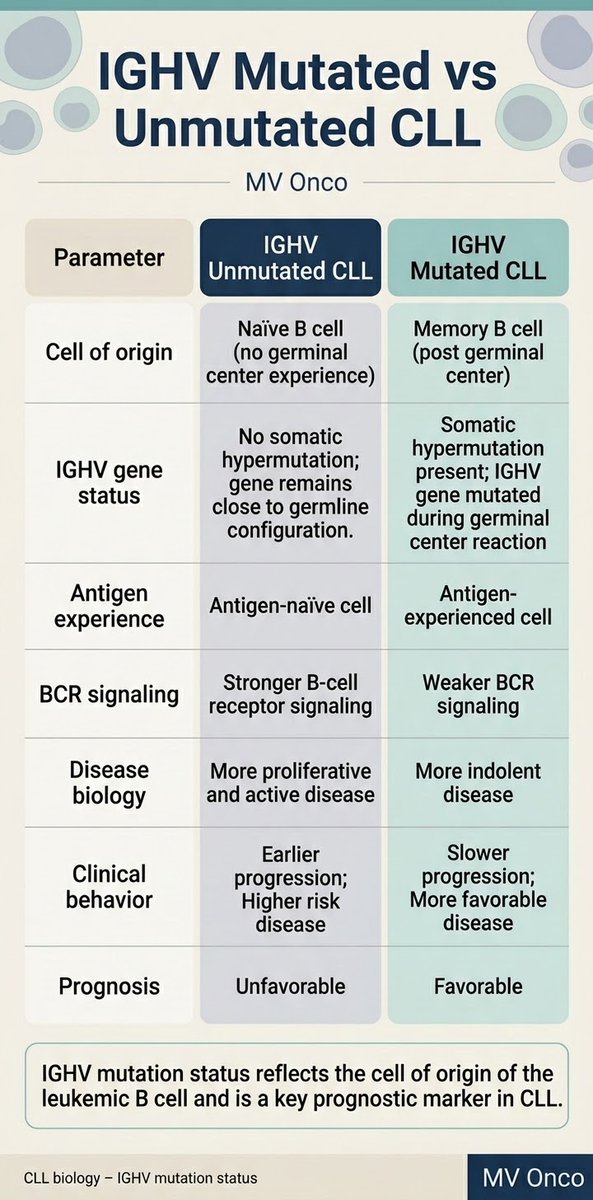
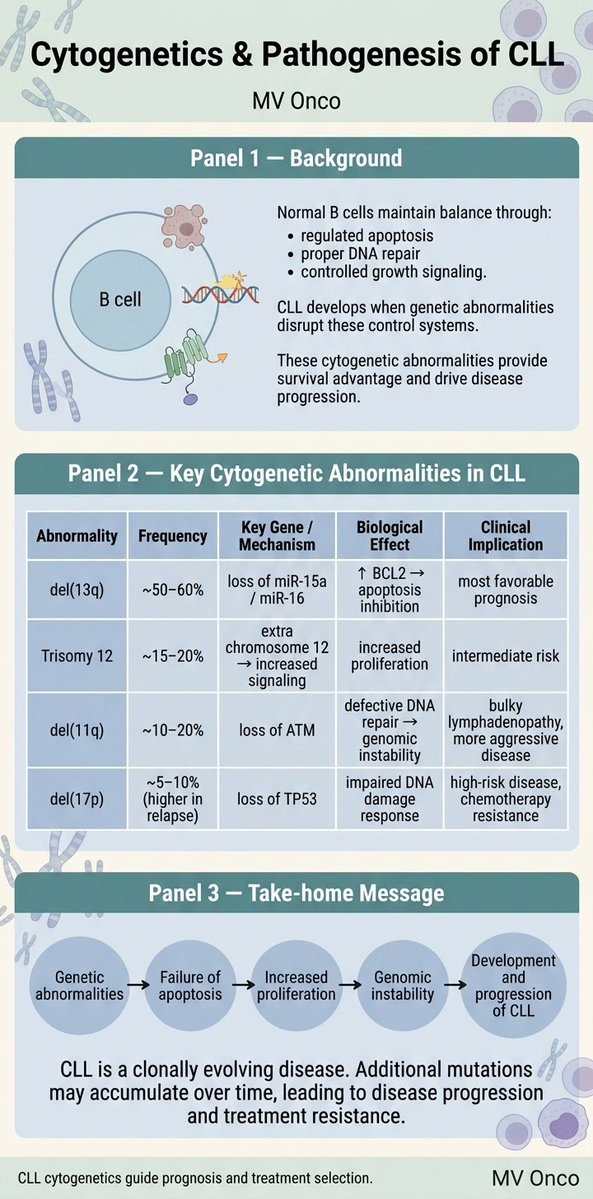
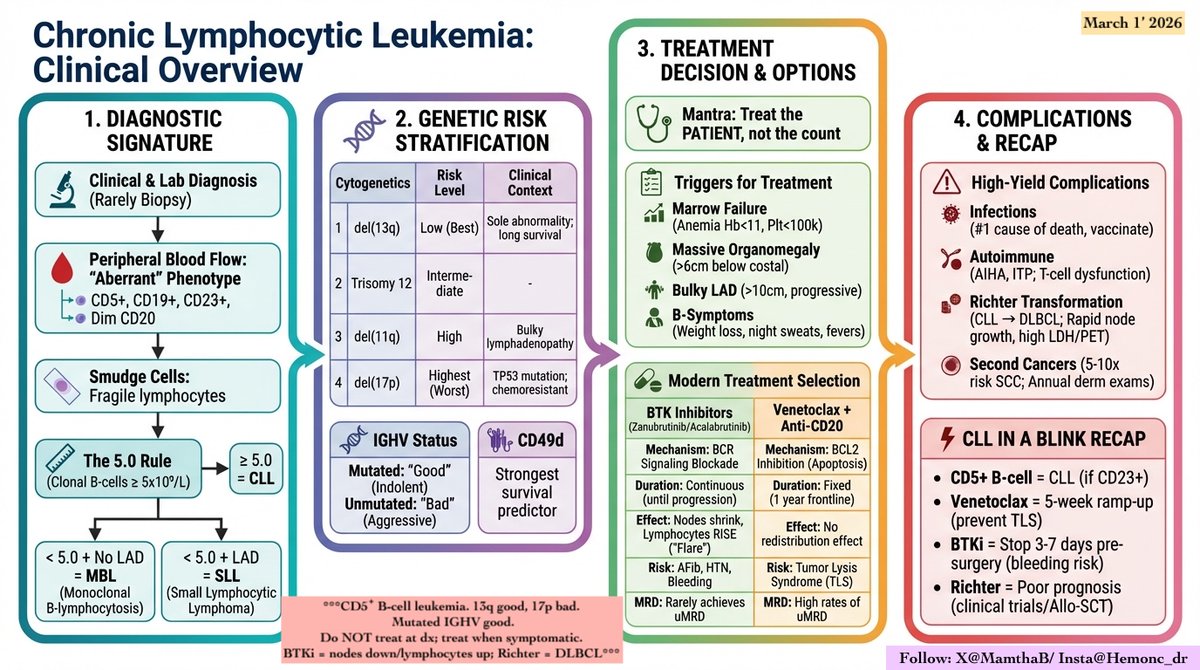
del(17p) vs TP53 mutation in CLL
They are related but not identical.
• 17p = chromosomal location
• TP53 = gene
• p53 = protein
Both disrupt the p53 tumor-suppressor pathway and predict chemo resistance.
Always test FISH + TP53 sequencing before therapy.
#MVOnco#CLL#HemOnc
Not all GI infections look the same under the microscope. 🔬
Knowing the size, staining, and epithelial location helps differentiate key coccidian parasites.
#Pathology#GITPathology#Parasitology #PathologyPearls#MedicalEducation #NEETSS#FRCPath #PathologyMCQ#Histopathology
Join me as I go live on pathCast to discuss recent practice related recommendations from GUPS and ISUP on diagnosis, grading and reporting of intraductal carcinoma of the prostate https://t.co/3P8qRyhkFo
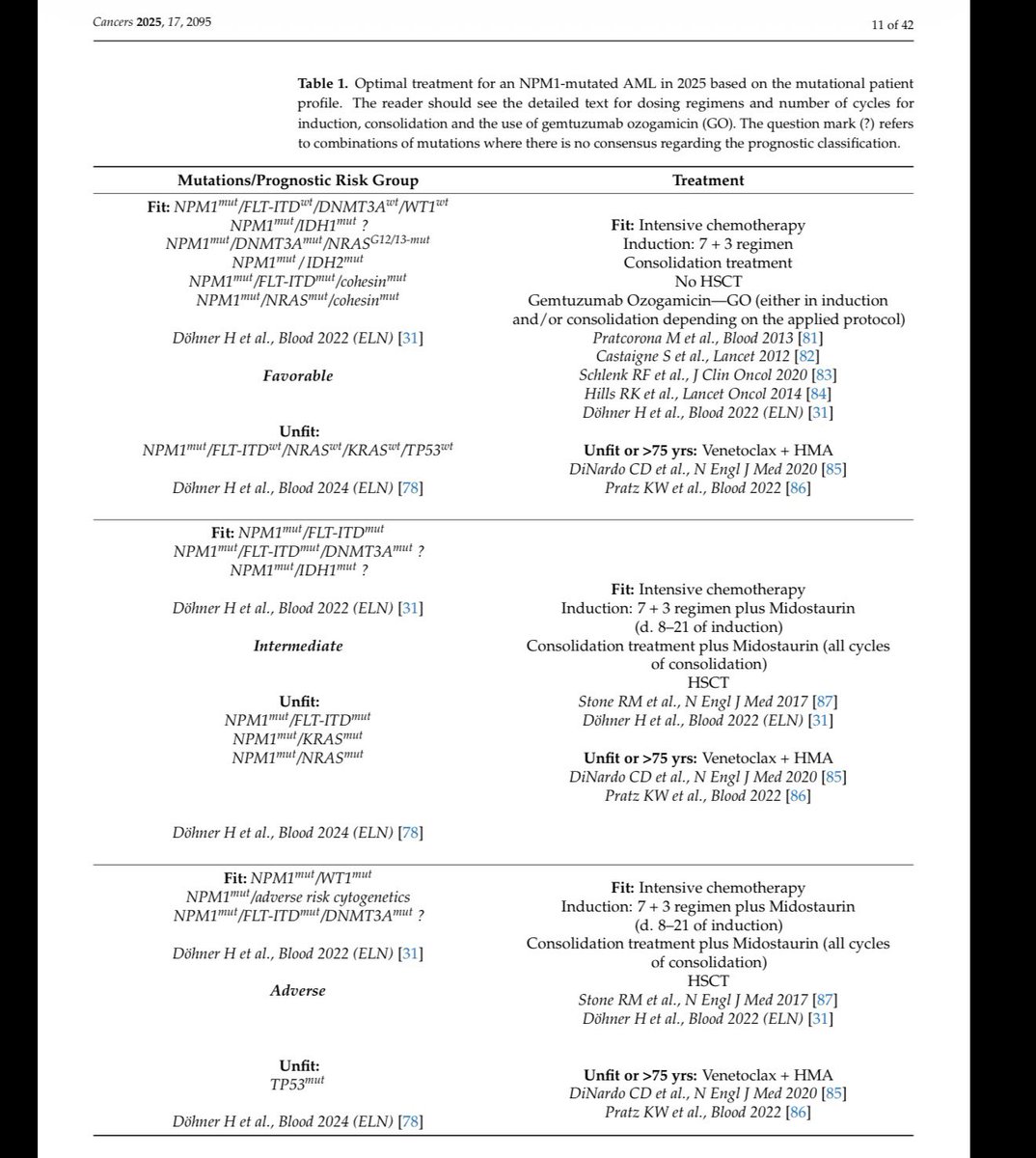
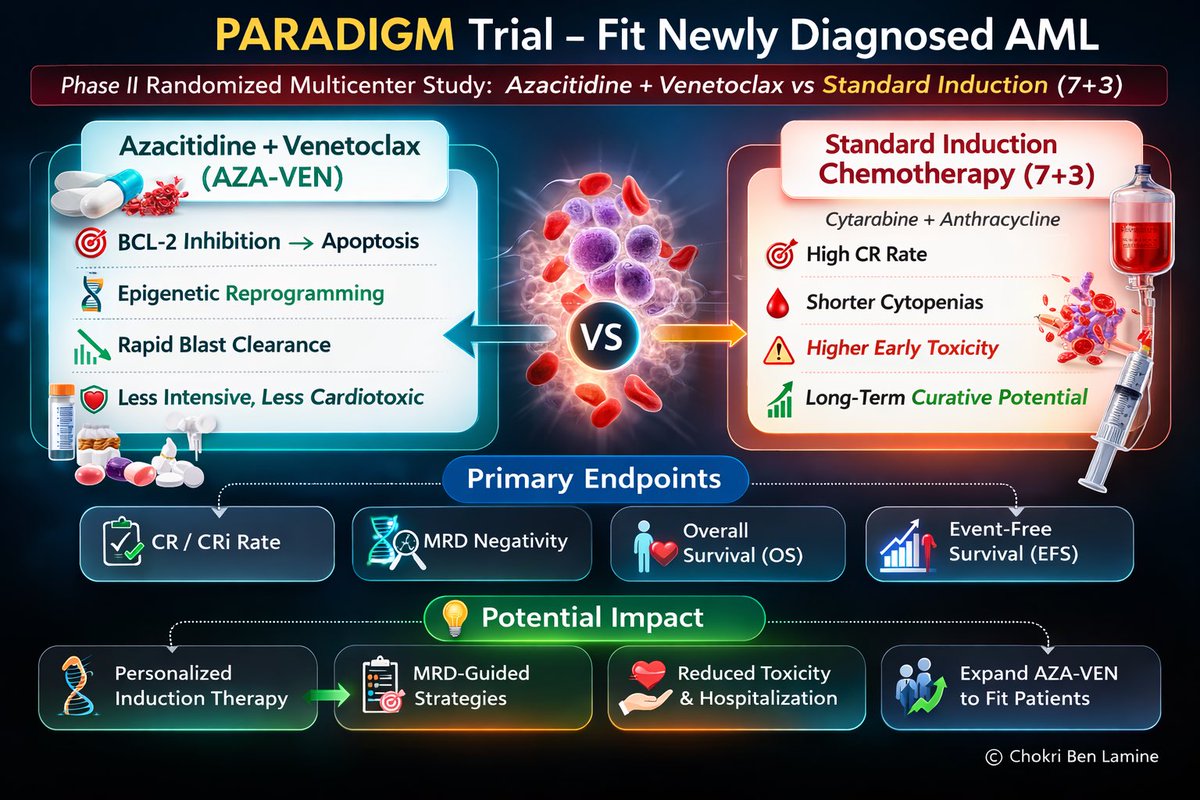
🧬 PARADIGM Trial — Azacitidine + Venetoclax vs Intensive Chemotherapy in Fit Newly Diagnosed AML
(Phase II randomized multicenter study)
⸻
🧵 50 High-Yield Pearls (Tweet-Style with Emojis)
1️⃣ 🧬 PARADIGM trial explores if AZA + VEN can replace intensive induction in fit newly diagnosed AML.
2️⃣ 🎯 Standard of care for fit AML remains 7+3 induction → high CR but significant toxicity.
3️⃣ 💊 Azacitidine + Venetoclax previously revolutionized therapy for unfit/elderly AML.
4️⃣ ❓ Key question: Can AZA-VEN work in younger fit AML patients?
5️⃣ 🧪 Phase II randomized multicenter trial.
6️⃣ 👥 Population: Newly diagnosed adult AML considered fit for intensive therapy.
7️⃣ ⚖️ Randomization:
AZA-VEN vs standard induction chemotherapy.
8️⃣ 🧬 Venetoclax → BCL-2 inhibitor causing mitochondrial apoptosis.
9️⃣ 🧫 Azacitidine → hypomethylating agent restoring tumor suppressor gene expression.
🔟 💥 Combination synergy: epigenetic reprogramming + apoptotic priming.
11️⃣ 🧪 Primary endpoint: CR/CRi rate.
12️⃣ 📊 Secondary endpoints: OS, EFS, MRD negativity, safety.
13️⃣ 🔬 MRD assessment increasingly used in AML response evaluation.
14️⃣ 🧠 Venetoclax is particularly effective in IDH-mutated AML.
15️⃣ 🧬 Also active in NPM1-mutated AML.
16️⃣ 📉 Historically lower activity in TP53-mutated AML.
17️⃣ ⚠️ Intensive chemo remains superior for FLT3-mutated AML when targeted therapy added.
18️⃣ 🧪 AZA-VEN produces rapid blast clearance.
19️⃣ ⏱ Response typically occurs within first 1–2 cycles.
20️⃣ 🧫 Bone marrow aplasia often occurs during therapy.
21️⃣ 🩸 Prolonged cytopenias are common toxicity.
22️⃣ 🦠 Infection risk remains major complication.
23️⃣ ⚕️ Careful antimicrobial prophylaxis required.
24️⃣ 💊 Venetoclax requires dose adjustment with azole antifungals.
25️⃣ 📉 Tumor lysis risk in AML is lower than in CLL but still monitored.
26️⃣ 🔬 MRD negativity correlates with longer survival outcomes.
27️⃣ 🧠 Non-intensive therapy may allow better tolerability in selected fit patients.
28️⃣ 📊 Trial evaluates whether remission depth equals that of chemotherapy.
29️⃣ 🧪 Key clinical debate: efficacy vs durability of response.
30️⃣ ⚖️ Intensive chemotherapy still offers long-term curative potential.
31️⃣ 🧬 Allo-SCT remains critical consolidation strategy.
32️⃣ 🧪 Venetoclax regimens increasingly used as bridge to transplant.
33️⃣ 🧠 Molecular subtype likely influences response.
34️⃣ 🔬 MRD-guided strategies may emerge from such trials.
35️⃣ 🧫 Venetoclax regimens show high CR rates in older AML (~65–70%).
36️⃣ 📉 Toxicity profile generally less cardiotoxic than anthracycline regimens.
37️⃣ ⚕️ Hospitalization duration may be shorter with AZA-VEN.
38️⃣ 🩺 Early mortality may be lower than intensive induction.
39️⃣ 🧪 However cytopenias often prolonged compared with chemotherapy.
40️⃣ 🔬 Resistance mechanisms include BCL-XL upregulation and mitochondrial adaptation.
41️⃣ 🧬 Combination strategies under investigation:
VEN + targeted inhibitors.
42️⃣ 💊 Trials evaluating VEN + FLT3 inhibitors.
43️⃣ 🧪 Also VEN + IDH inhibitors.
44️⃣ 🧬 Personalized AML therapy increasingly genomics-driven.
45️⃣ ⚖️ PARADIGM contributes to debate:
Should all AML patients receive intensive therapy?
46️⃣ 🧠 Fit status alone may not determine optimal therapy.
47️⃣ 📊 MRD-guided adaptive therapy likely future paradigm.
48️⃣ 🧪 Non-intensive therapy may expand frontline AML options.
49️⃣ 🔬 Final interpretation depends on survival outcomes vs CR rate.
50️⃣ 🚀 Trial represents step toward precision-tailored induction therapy in AML.