🔱Segunda Definición Universal de Insuficiencia Cardíaca (AHA/ACC/ESC/WHF 2026). 🫀
🔶️La IC es un síndrome clínico caracterizado por síntomas y/o signos típicos, secundarios a una anormalidad estructural o funcional cardíaca, cuya certeza diagnóstica se fortalece con niveles elevados de péptidos natriuréticos (BNP o NT-proBNP) y/o evidencia objetiva de congestión o aumento de presiones de llenado mediante estudios de imagen (Eco).
🔶️Se abandona la clasificación basada en puntos de corte rígidos de FEVI. La IC se agrupa ahora en FE reducida, FE preservada y FE mejorada, priorizando el contexto clínico.
🔶️Se incorpora una clasificación universal por etiología, promoviendo la identificación de causas específicas (isquémica, hipertensiva, valvular, infiltrativa, genética, inflamatoria, tóxica, metabólica, entre otras) para orientar un tratamiento más preciso.
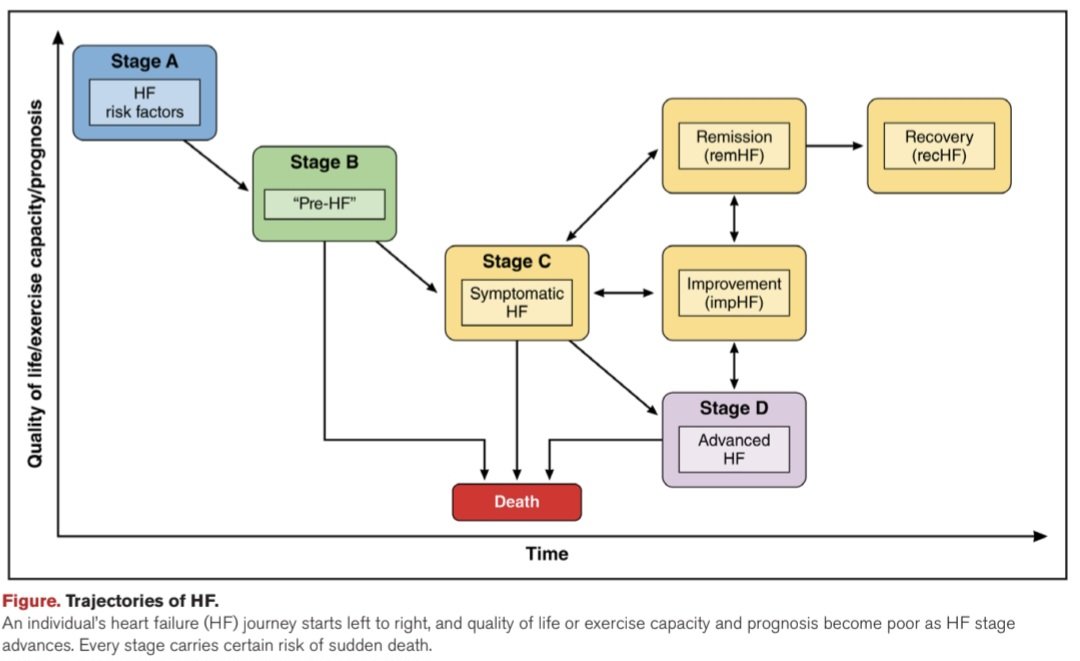
🔶️Se fortalece el concepto de prevención, resaltando la identificación y tratamiento de los estadios A (riesgo) y B (preinsuficiencia cardíaca) antes de la aparición de síntomas.
🔶️Se introduce el concepto de trayectorias de la enfermedad: mejoría, remisión y recuperación.
📄🆓️⤵️ @AHAScience 💯
DOI: 10.1161/CIR.0000000000001455
https://t.co/At2Ctq2FsA
🫁Weaning from mechanical ventilation is not “turn down pressure support.”
It is a structured test of whether the patient can breathe, protect the airway, and survive extubation.
Recent PubMed indexed guidelines emphasize daily readiness screening and spontaneous breathing trials once the cause of respiratory failure is improving, oxygenation is acceptable, hemodynamics are stable, sedation is light, cough is adequate, secretions are manageable, and mental status allows airway protection (Roberts et al., 2024; Ha et al., 2024).
Classic parameters still matter:
RSBI
Respiratory rate
Tidal volume
Minute ventilation
NIF or MIP
Cough strength
Gas exchange
pH and PaCO₂
Hemodynamic response
Work of breathing
Secretion burden
But no single number should decide extubation.
Ultrasound adds physiology. Diaphragm excursion and thickening fraction predict weaning success with reasonable accuracy, but heterogeneity is high, so ultrasound should complement, not replace, clinical assessment (Parada-Gereda et al., 2023). Lung ultrasound helps detect loss of aeration, pulmonary edema, pleural effusion and post-extubation risk. Cardiac ultrasound is essential when weaning failure may be cardiac.
Special populations need phenotype-based weaning.
COPD: avoid excessive support reduction, monitor dynamic hyperinflation, auto-PEEP, pH and CO₂; extubation to NIV is often appropriate.
Heart failure: SBT increases venous return and LV afterload; look for B-lines, rising filling pressures, mitral inflow changes, hypertension and weaning-induced pulmonary edema.
Obesity: higher work of breathing, atelectasis and OSA risk; optimize positioning, PEEP, recruitment, and consider NIV or CPAP after extubation.
Prolonged ventilation and frailty: search for weakness, malnutrition, delirium, diaphragm dysfunction, poor cough and rehabilitation needs (Shah et al., 2024).
References 📚
Ha, T. S.. Acute and Critical Care, 39(1), 1–23. https://t.co/nEKBaNAUTu
Parada-Gereda, H. M. Critical Care, 27, 174. https://t.co/YwZf3dQpBZ
Roberts, K. J. Respiratory Care, 69(7), 891–901. https://t.co/8qjofP721j
Shah, N. M. Breathe, 20(3), 240122. https://t.co/sSUC0KLsww
Today's Paper of the Day is:
Hyperangulated videolaryngoscopy
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026
Adult Circulatory Support
Hemodynamic Considerations of Distal Perfusion Catheters With Venoarterial Extracorporeal Membrane Oxygenation: A Dynamic Mock Loop Study
ASAIO Journal 72(6):p 439-448, June 2026
https://t.co/eJIV9CCgxw
#ASAIO#ECMO#perfusion#CirculatorySupport
🧠 Are We Missing Half of the Brain's Circulation?
For decades, neurocritical care has focused primarily on arterial flow.
We monitor cerebral perfusion, vasospasm, autoregulation, pulsatility indices, and intracranial pressure. Yet one critical component of intracranial hemodynamics remains largely overlooked:
Cerebral venous outflow.
A recent review in Diagnostics argues that Transcranial Color Doppler (TCCD) should evolve beyond being merely the "stethoscope of the brain" for arterial circulation and begin incorporating systematic assessment of cerebral venous drainage.
The authors highlight a simple but important physiological concept:
🩸 Intracranial hypertension is not only a problem of arterial inflow.
It may also be a problem of impaired venous outflow.
Mechanical ventilation, elevated PEEP, hypercapnia, increased intra-abdominal pressure, Trendelenburg positioning, cardiac tamponade, pulmonary hypertension, large-bore jugular catheters, and venous obstruction can all impair cerebral venous drainage and contribute to cerebral congestion.
Using venous TCCD combined with internal jugular vein ultrasound, clinicians may be able to detect cerebral venous congestion before conventional markers such as optic nerve sheath diameter (ONSD) enlargement or arterial Doppler changes become evident.
Particularly interesting for intensivists and anesthesiologists, the review presents clinical examples where:
🔹 Mechanical ventilation reduced Rosenthal vein flow despite stable arterial Doppler findings.
🔹 Large-bore central venous catheters further impaired cerebral venous drainage.
🔹 Hemodynamically significant pericardial effusion produced profound venous congestion detectable by ultrasound before definitive diagnosis.
🔹 Pneumoperitoneum and Trendelenburg positioning increased jugular venous congestion during surgery.
The key message is not that venous TCCD replaces current neuromonitoring tools.
Rather, it may provide an additional physiological layer that helps explain why some patients develop intracranial hypertension despite apparently acceptable arterial parameters.
As critical care increasingly moves toward physiology-guided management, perhaps the next frontier is understanding not only how blood enters the brain, but also how it leaves it.
Question for the neurocritical care and perioperative community:
Do you routinely consider cerebral venous drainage when adjusting PEEP, patient positioning, pneumoperitoneum pressures, or central venous access strategies?
Reference📚
Bianchini A, Vitale G, Melegari G, et al. Transcranial Color Doppler for Assessing Cerebral Venous Outflow in Critically Ill and Surgical Patients. Diagnostics. 2026;16:289.
https://t.co/S4Hy5iDXf0
#NeurocriticalCare #POCUS #TCD #TCCD #CriticalCare #IntensiveCare #Anesthesiology #NeuroMonitoring #Ultrasound #MechanicalVentilation #ICP #BrainInjury #CriticalCareMedicine #FOAMed #MedEd
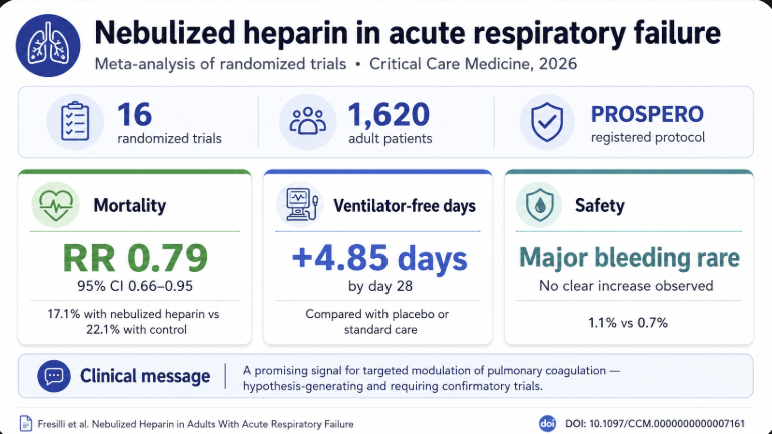
New in @CritCareMed: our meta-analysis of 16 RCTs (1,620 adults) suggests nebulized heparin in acute respiratory failure may lower mortality (RR 0.79, 95% CI 0.66–0.95) and increase ventilation-free days, with no safety signal. https://t.co/PcEnM7kpEn
One liter of air. One hour. No catastrophe.
If venous air enters slowly, the lungs can act as a powerful filter and reabsorb it.
But push the rate beyond ~1.5 L/hour, and the filter may fail: bubbles can cross into the left circulation — where the real danger begins.
🫁🤰🏼Respiratory failure in late pregnancy remains one of the most physiologically complex scenarios in critical care medicine.
The paper elegantly explains how:
• Functional residual capacity decreases by up to 30%
• Oxygen consumption increases significantly
• Minute ventilation rises chronically through progesterone mediated respiratory drive
• The diaphragm is displaced upward
• Chest wall elastance increases in late gestation
• The maternal PaCO₂ set point physiologically falls to approximately 28-32 mmHg
This creates an extremely narrow physiological reserve.
One of the strongest sections of this review is the discussion of maternal-foetal gas exchange.
The fetus is completely dependent on maternal oxygenation AND uteroplacental perfusion.
This means: Maternal hypoxaemia, hypotension, excessive PEEP, hypercapnia, or severe vasoconstriction can directly compromise fetal oxygen delivery.
Importantly, the authors challenge the simplistic application of conventional ARDS strategies to obstetric critical care.
The review also provides an excellent mechanistic explanation of why patient self inflicted lung injury (P-SILI) may be particularly dangerous in late pregnancy.
Pregnancy already exists in a state of:
• Elevated respiratory drive
• Increased minute ventilation
• Reduced FRC
• Increased inspiratory effort requirements
Once lung injury develops, vigorous spontaneous inspiratory efforts can generate excessive transpulmonary pressures and pendelluft phenomena, amplifying lung injury.
This has major implications for:
• Timing of intubation
• Sedation strategy
• Monitoring inspiratory effort
• Neuromuscular blockade decisions
The article reinforces an increasingly important message: Pregnancy itself is NOT a contraindication for prone positioning nor VV ECMO.
With proper support of the gravid uterus, multidisciplinary coordination, and fetal monitoring:
• Full prone positioning can be safely performed
• Semi prone approaches are feasible
• ECMO survival has improved substantially, approaching ~75% maternal survival in experienced centers
This is not simply obstetric medicine.
It is advanced cardio-pulmonary physiology under extreme adaptive stress.
Perhaps the most important practical message from this review is this:
In critically ill pregnant patients, optimal maternal physiology IS fetal resuscitation.
The goal is not “protecting the fetus instead of the mother.”
The goal is aggressive maternal stabilization using physiology adapted to pregnancy.
📚Williams K, White A, Nana M, et al. Managing Respiratory Failure in Late Pregnancy. Journal of Clinical Medicine. 2026;15(9):3449. doi:10.3390/jcm15093449
Central venous oxygen saturation vs. oxygen extraction ratio in septic shock resuscitation: Which metric is more informative?
CCR Journal Watch
https://t.co/Sp06oA6IDG
Today's Paper of the Day is:
A narrative review of the diabetic ketoacidosis and hyperosmolar hyperglycemic state overlap syndrome
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026
🫀🤓Pressure does not move blood. Energy does.
This outstanding review challenges one of the most deeply rooted concepts in haemodynamic management: the idea that pressure variables are the primary drivers of circulation. Instead, the authors propose a physiology framework where the heart supplies energy, the vasculature defines constraints, and pressures merely reflect system state.
Several concepts deserve special attention for critical care clinicians:
• Mean systemic pressure does not “drive” flow
• Right atrial pressure is a dependent variable, not a therapeutic target
• Venous return depends on inflow acceptance and inlet impedance
• Raising pressure without improving flow may worsen congestion
• Shock should be interpreted as either impaired venous delivery or impaired cardiac acceptance
Clinically, this framework helps explain why:
• CVP-guided fluid loading often fails
• Vasopressors may normalize MAP without restoring perfusion
• Congestion can coexist with preserved arterial pressure
• Flow responsiveness matters more than static pressure targets
One of the strongest messages of the paper is simple but powerful:
“Pressure is not perfusion.”
For intensivists, anesthesiologists, and cardiogenic shock teams, this review is worth reading in full. It reconnects bedside haemodynamics with first-principles physiology.
Miller A, Anaesthesia. 2026. https://t.co/ejjvREUe7c
Today's Paper of the Day is:
Remote ischemic conditioning in intensive care: From bench to bedside
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026
Today's Paper of the Day is:
Acute Respiratory Distress Syndrome and Fluid Management: Finding the Perfect Balance
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026
FLIGHT-to-ECPR study: Helicopter-EMS-facilitated hospital-based #ECPR to expand access to #ECMO in CA?? Low-flow times frequently extended in rural settings!
🚁 45 adults with refractory VF/VT OHCA
🩸 60% ECPR, low-flow = 86'±29
🧠 overall favourable neurologic survival 33%: 26% in ECPR, 44% if no cannulation
In matched ECPR patients, similar low-flow times, same favourable survival. No differences in cannulation performance, run duration, LoS.
HEMS-facilitated strategy feasible & safe to expand access to advanced resuscitation beyond traditional urban areas. Geography alone should not preclude ECPR when timely reperfusion can be maintained.
@ResusJournal
🔓 https://t.co/UbEgP226pT
🫀Valvular cardiogenic shock is probably one of the most underrecognized phenotypes of shock in modern cardiac critical care.
What makes this paper particularly important is that it reframes severe valve disease:
not as chronic structural cardiology, but as acute hemodynamic catastrophe.
The physiology is brutal.
Unlike classic ischemic CS, VCS often combines:
🫀 abrupt preload overload
🫀 severe afterload mismatch
🫀 elevated filling pressures
🫀 pulmonary edema
🫀 impaired forward flow
🫀 rapidly collapsing ventriculo arterial coupling
And unlike MI related shock: 📌 many of these patients still have relatively preserved LVEF.
Which means: normal or “acceptable” EF does NOT exclude severe shock physiology.
One of the most fascinating findings: 📌 the aortic valve was the most commonly involved valve.
Especially: • aortic stenosis • acute aortic regurgitation
And outcomes differed substantially by lesion type.
Patients with:
⚠️ stenotic lesions had the worst survival
⚠️ regurgitant lesions performed better
⚠️ mixed lesions remained intermediate
Severe AS in shock creates:
• fixed forward flow obstruction
• catecholamine inefficiency
• coronary hypoperfusion
• profound ventriculo arterial uncoupling
while acute regurgitant lesions may still preserve some forward stroke volume if rapidly corrected.
Another extremely important message:
📌 definitive intervention mattered enormously.
Compared to medical therapy alone:
• surgery had the best survival
• percutaneous therapies were intermediate
• medical management had the worst outcomes
After multivariable adjustment: medical management alone was associated with nearly 4 times higher hazard of death at 1 year.
But this study suggests: ⚡ definitive therapy may be the only real survival strategy.
The paper also highlights something increasingly relevant for modern CICUs:
📌 prosthetic valve dysfunction accounted for almost one third of VCS cases.
With aging populations and expanding TAVR/bioprosthetic use: this phenotype will likely increase dramatically over the next decade.
From a hemodynamic perspective, VCS may require:
🩺 earlier invasive monitoring
🩺 advanced echocardiography
🩺 rapid valve team activation
🩺 individualized MCS strategy
🩺 faster transfer to high volume structural centers
The study also indirectly supports something many intensivists already suspect:
📌 timing is probably everything.
Delayed recognition likely converts salvageable hemodynamic collapse into irreversible multiorgan failure.
This is where future research should probably focus:
• shock phenotyping by valve lesion
• optimal MCS selection
• VA coupling analysis
• transcatheter rescue timing
• CICU to structural heart pathways
• predictive models for intervention candidacy
📖 Nair RM, JACC Advances. 2024;3(11):101303.
https://t.co/eo9wstNwiZ
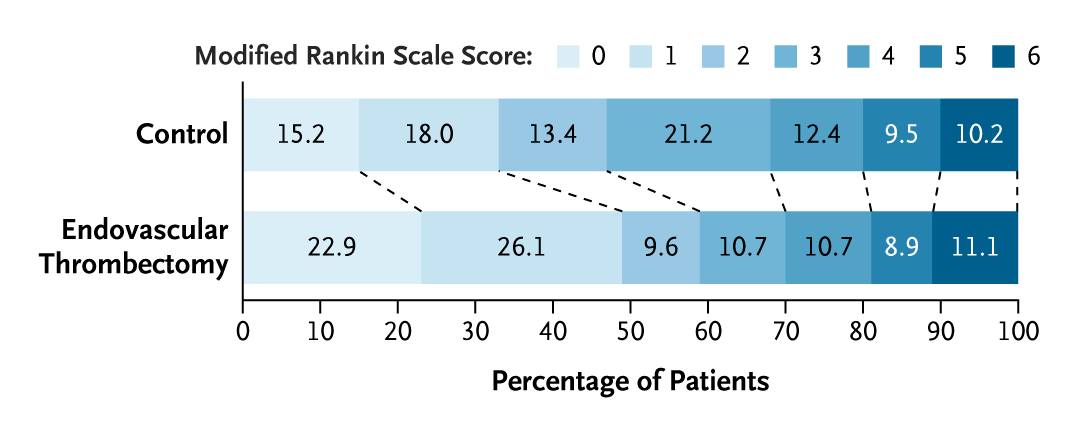
Original Article: Endovascular Treatment of Medium-Vessel-Occlusion Strokes (ORIENTAL-MeVO trial) https://t.co/sa2YKbUb6G
Editorial: Endovascular Therapy for Medium-Vessel Occlusion Stroke — Narrowing the Target Population https://t.co/UBLyNvnu8M
#Neurology