Dear friends, as promised, the citizens funded generics vs. branded drugs project is now published after 4 months in peer review. It was hardwork, but worth the effort because all of you helped us realize this important work.
You can read the full detaild paper here: https://t.co/jZhm8ZcPCq
Here is a simplified summary:
Do cheaper generic medicines work as well as expensive branded ones? It's a question that worries patients and even many doctors, who often quietly assume that a low price must mean lower quality. This doubt has real consequences in India, where medicines make up nearly two-thirds of what families spend out of their own pockets on healthcare — a burden that pushes millions into poverty and forces people to split doses or stop treatment altogether.
To put the question to a fair, independent test, our team at the Mission for Ethics and Science in Healthcare (MESH) carried out a fully citizen-funded study, paid for entirely by donations from ordinary members of the public, with no money or influence from any drug company.
We bought 131 samples of 22 commonly used medicines — covering heart disease, diabetes, infections, pain, acidity, and more — from seven different kinds of outlets across Kerala, including government stores like Jan Aushadhi, private generic chains, and premium branded pharmacies. Every sample was then coded, blinded, and sent to a top accredited laboratory for rigorous testing against the Indian Pharmacopoeia 2022 standards. What makes this study unusual is that very few before it have tested branded and generic versions from the same market side by side, included government-supplied medicines, and combined strict quality testing with a hard look at price — all at the same time.
The result was striking in its simplicity: every single one of the 131 medicines passed every quality test. 100%. It made no difference whether a pill was generic or branded, cheap or expensive — they were all equally good in their active ingredient content, their purity, and how they dissolve in the body.
Yet the prices told a completely different story. Generic medicines were, on average, 48.6% cheaper than their branded twins, and the most expensive brand cost up to 13.9 times more than the cheapest generic of the very same drug. Government Jan Aushadhi stores were the cheapest source for 18 of the 22 medicines tested, with potential savings running into thousands of rupees a year per medicine — for instance, over ₹16,000 a year on a single liver drug.
For doctors, this is reassuring, hard evidence that prescribing a quality-assured generic is not a compromise on care; it is the same medicine at a fraction of the cost. For patients, it means you can stay on your treatment without it draining your savings, which is exactly what keeps people healthier over the long run.
And this is precisely why independent, publicly funded projects like this matter so much for the future of healthcare in India: they answer the questions ordinary people actually have, free from commercial pressure, and they build the trust that programmes like Jan Aushadhi need to truly succeed. Affordable and high-quality are not opposites — in a well-regulated market, they go hand in hand.
More here: https://t.co/jZhm8ZcPCq
Huawei’s Pura 90 series comes with AI Posture Recommendations for better photos.
THIS is how AI is supposed to be used.
Yea, it’s way more useful than Google’s camera coach slop.
30 days ₹18000 stipend countless harassment and threats i still continued till the end of the journey This experience has definitely made me somewhat blackpilled.
A final-year law student, Rishi Kumar from Tamil Nadu National Law University, refuses to delete his blog criticising the Supreme Court… despite pressure from his own university.
Why?
Because the administration allegedly received calls from advocates, judges, and others claiming the post harms the institution’s “reputation.”
The blog titled “The Supreme Court of India Has No Spine” questioned the court’s decision to ban an NCERT textbook chapter on judicial corruption.
But here’s the real issue:
A law student is being told to silence himself… for expressing a legal opinion.
His response?
Clear and powerful:
“My opinions are mine… you do not own my voice or my conscience.”
He even said he’s ready to face disciplinary action rather than back down.
This isn’t just about one blog.
This is about academic freedom vs institutional pressure.
If law students… the future of the judiciary are discouraged from questioning the system,
then who exactly is allowed to question it?
Criticism of institutions ≠ disrespect.
Silencing criticism = weakening democracy.
Have received notice from Kerala police for the tweet below. Kerala Police in the notice said the tweet insults the election commission of India and propagate content that undermines communal harmony.
Scammed for ₹2.9L on @AmazonIN. Ordered a GIGABYTE RTX 5090 for our startup, received 1kg of Ghadi detergent. This was "Fulfilled by Amazon" (FBA), meaning it was stored and shipped directly from an Amazon warehouse. @AmazonHelp#AmazonScam#ConsumerRights [more in thread]
That’s pretty disgraceful. In a democracy, screening a film is a reflection of our society’s freedom of expression and has nothing to do with government to government relations. This practice of banning films or books because of the offence they might cause to foreign countries must stop immediately. It’s unworthy of a mature democracy. #HindRajab
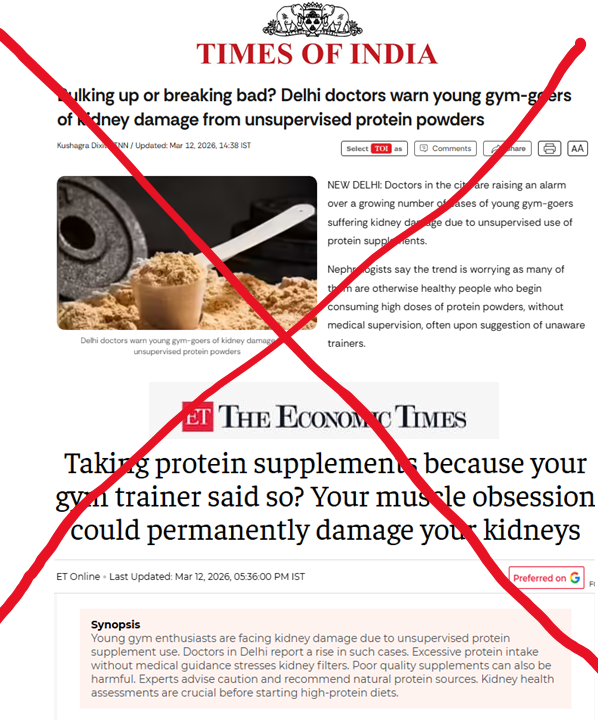
Extremely irresponsible reporting by @TOIIndiaNews and @EconomicTimes. I do not know what the crtieria for being your "health reporter" is, but this feels like some kid in 12th grade doomscrolling conspiracy theories on Instagram wrote it. Do better.
Here are the rebuttals to the nonsense your so-called kidney experts and health journalist spouted in the article:
The title claim: "Protein supplements could permanently damage your kidneys"
This is fear-mongering presented as fact.
Multiple systematic reviews and meta-analyses (including a 2018 meta-analysis in the British Journal of Sports Medicine) have found no evidence that protein supplementation causes kidney damage in people with normal renal function. The International Society of Sports Nutrition position stand on protein safety states that intakes of 1.4–2.0 g/kg/day are safe for healthy, exercising individuals, with some data supporting up to 3.4 g/kg/day over extended periods without adverse renal effects. Even the "Gym Nephropathy" review in the Journal of the Egyptian Society of Nephrology and Transplantation concedes that high protein intake improves training adaptations with no harm when baseline renal function is normal.
The word "permanently" in the title has no basis in the literature for whey protein in healthy kidneys.
Conflation of whey protein with anabolic steroids, cough syrups, growth hormone, alcohol, and nicotine
This is the most intellectually dishonest move in this article. The cited case reports invariably involve young men using anabolic-androgenic steroids (AAS), diuretics, banned substances like spasmo-proxyvon, cough syrups (containing dextromethorphan or codeine for abuse), and sometimes alcohol — alongside protein. The kidney damage in these cases is driven by AAS-induced FSGS (focal segmental glomerulosclerosis), injury from stimulant abuse, or direct kidney damage from banned drugs. Blaming the whey protein powder in this cocktail is like blaming the glass of water someone drank alongside the poison.
Whey protein is not a "gym supplement" in the same category as testosterone injections or codeine-containing cough syrups, and lumping them together under the umbrella "gym supplements" is a category error designed to maximise alarm.
Excessive protein intake causes hyperfiltration injury to the kidney filters
Hyperfiltration is a normal physiological adaptation, not abnormal injury. When you eat more protein, kidney filtration increases to handle the increased nitrogen load — this is the kidney doing its job, just as heart output rises during exercise without "damaging" the heart.
The Brenner hypothesis (that hyperfiltration leads to progressive kidney damage) was derived from animal models of kidney disease and patients with chronic kidney disease or after kidney removal surgery, not from healthy kidneys. The conflation of "adaptive hyperfiltration" with "injurious hyperfiltration" is a basic error in renal physiology.
The Nephrologists cited in the article should go back to first year MBBS.
The case report: 20-year-old with kidney damage
This is the centrepiece of the article, and it's doing enormous heavy lifting for very little information. We're told he had "no prior medical issues" but developed proteinuria and oedema after 6–8 months of consuming protein powders.
What we are NOT told: what else he was taking (steroids? pre-workouts? creatine at absurd doses? SARMs?), how much protein he was consuming, whether he had undiagnosed IgA nephropathy or FSGS (both common in young Indian males and often unmasked by any physiological stressor), whether a renal biopsy was performed, and what the histopathological diagnosis was.
A single uncontrolled case report with incomplete clinical details proves nothing about causation. The fact that his parents are doctors is irrelevant to the pathology but is included for emotional impact — classic journalistic manipulation.
The infographic claim: "Most healthy adults need only ~0.8 g protein per kg body weight/day"
This is the RDA — the Recommended Dietary Allowance — which represents the minimum intake to prevent clinical protein deficiency in sedentary adults. It is not a ceiling. It is not optimal. It is the bare minimum to avoid malnutrition. For resistance-training individuals (which is the population this article targets), 0.8 g/kg/day is inadequate to support muscle protein synthesis and recovery. Presenting the sedentary minimum as the recommended ceiling for gym-goers is either ignorance of sports nutrition or deliberate fear-mongering.
Dr Ravi Bansal: "individuals should avoid exceeding a protein intake of 1.2 g/kg of body weight"
This is a nephrologist speaking from a CKD-management perspective and inappropriately generalising it to healthy gym-goers. The 1.2 g/kg figure is the upper limit sometimes recommended for patients with established mild-to-moderate CKD (stages 2–3) to slow progression. It has no applicability to healthy young adults with normal renal function who are resistance training.
Dr Bansal: "natural dietary proteins remain superior to artificial substitutes"
Whey protein is not an "artificial substitute." It is derived from milk through a physical separation process (filtration). It contains the same amino acids as the protein in a glass of milk, yoghurt, or paneer. Calling it "artificial" is factually wrong and plays into the naturalistic fallacy that pervades Indian health discourse — the same fallacy that props up Ayurvedic products with actual hepatotoxic potential while demonising a dairy-derived food product. There is no evidence that protein from whey is metabolised differently or has different renal effects compared to protein from chicken, eggs, or lentils at equivalent doses.
This report cherry-picks a single incomplete case report, conflates physiological adaptation with pathological injury, misrepresents the RRecommended Daily Allowance as a maximum safe intake, ignores the actual evidence from controlled trials and meta-analyses, lets steroid abuse and supplement contamination off the hook entirely, and wraps it all in World Kidney Day alarmism.
This is irresponsible health journalism in a country where protein deficiency kills far more people than protein excess ever has.

















![beingcarrot's tweet photo. Scammed for ₹2.9L on @AmazonIN. Ordered a GIGABYTE RTX 5090 for our startup, received 1kg of Ghadi detergent. This was "Fulfilled by Amazon" (FBA), meaning it was stored and shipped directly from an Amazon warehouse. @AmazonHelp #AmazonScam #ConsumerRights [more in thread] https://t.co/NfgUL0jmvL](https://pbs.twimg.com/media/HEBat6bboAERysa.jpg)
![beingcarrot's tweet photo. Scammed for ₹2.9L on @AmazonIN. Ordered a GIGABYTE RTX 5090 for our startup, received 1kg of Ghadi detergent. This was "Fulfilled by Amazon" (FBA), meaning it was stored and shipped directly from an Amazon warehouse. @AmazonHelp #AmazonScam #ConsumerRights [more in thread] https://t.co/NfgUL0jmvL](https://pbs.twimg.com/media/HEBas3gbAAAiU2c.jpg)
![beingcarrot's tweet photo. Scammed for ₹2.9L on @AmazonIN. Ordered a GIGABYTE RTX 5090 for our startup, received 1kg of Ghadi detergent. This was "Fulfilled by Amazon" (FBA), meaning it was stored and shipped directly from an Amazon warehouse. @AmazonHelp #AmazonScam #ConsumerRights [more in thread] https://t.co/NfgUL0jmvL](https://pbs.twimg.com/media/HEBapS_asAAZX-Y.jpg)






















![beingcarrot's tweet photo. Scammed for ₹2.9L on @AmazonIN. Ordered a GIGABYTE RTX 5090 for our startup, received 1kg of Ghadi detergent. This was "Fulfilled by Amazon" (FBA), meaning it was stored and shipped directly from an Amazon warehouse. @AmazonHelp #AmazonScam #ConsumerRights [more in thread] https://t.co/NfgUL0jmvL](https://pbs.twimg.com/media/HEBautGb0AAR1i5.jpg)