@Dr__Sarmy “ I have considered it, and am not prepared to issue this medication, but your consultant Psychiatrist, who will be very familiar with this medication, may wish to do so”
Celebrities, rich people and ex-prime ministers should not make health policy. Prostate cancer screening is just not as simple as some are making out. There are real harms caused when people are treated unnecessarily.
This week the NHS will undergo one of the most radical – and scandalous - changes in its history. From 1st April (the public are the fools in this), GPs will be contractually obliged to seek remote, electronic “advice and guidance” from hospital ‘clinicians’ (note, not necessarily doctors), making it even harder for patients to see a hospital specialist.
Does this sound part of a plan to genuinely ‘fix’ the NHS, as Wes Streeting vowed he would do so effusively when taking up office - or more like a tactic to ration hospital care by overriding GPs in order to massage the waiting list figures?
It is, of course, the latter, an extra layer of bureaucracy that at best will delay patients’ access to the specialist treatment they need, at worse sacrifice those patients on the altar of fake news about “falling” waiting lists.
You don’t need me to point out the patient safety risks it potentially entails. We all know that time, in medicine, can be everything. The Royal College of GPs has been crystal clear: “The use of advice and guidance should not be mandated in any area… We have heard reports of risks of delays, with tests being required before any referral, lost messages and staff without appropriate senior clinical oversight handling requests.”
The aim, says the Times, is to reduce the number of hospital outpatient appointments by 30 million annually. And the government, in a really quite breathtaking example of political spin, is presenting this as “good” for patients - as though all those people who’ve been waiting years months or even years for the first Rheumatology, Neurology or Orthopaedics appointment they so desperately need are just, you know, malingering. (I recently spoke to a patient with a new diagnosis of multiple sclerosis who’d been waiting over six months to see a neurologist for the first time – simply scandalous.)
I believe this is a national health scandal from a government that apparently cares more about good spin than it does about good patient care.
If you feel the same, please – please – write to your MP or the Secretary of State and tell them why. Please shout about this online, in the press, anywhere you can. Don’t let this slide. Thank you.
Oh god someone who doesn’t know chemistry or biochemistry
This is a classic chemistry fallacy—pretending that a substance is either “good” or “bad” regardless of dose, form, and exposure. Toxicology doesn’t work that way. As Paracelsus said centuries ago: “The dose makes the poison.”
Here’s the reality behind each of those comparisons:
Mercury
•Fish may contain methylmercury, a bioaccumulating neurotoxin that builds up in large predatory fish.
•Vaccines historically contained ethylmercury (thimerosal), which is metabolized and cleared quickly and is not the same compound.
•Today, most childhood vaccines contain no thimerosal at all.
Formaldehyde
•Used industrially in building materials at higher exposures.
•Tiny amounts are used during vaccine manufacturing to inactivate toxins or viruses, and only trace residual amounts remain.
•Your own metabolism produces far more formaldehyde naturally every day than any vaccine contains.
Glyphosate
•Agricultural herbicide.
•Not present in vaccines. The comparison is simply false.
Aluminum
•Aluminum salts are used in some vaccines as adjuvants to improve immune response.
•The amount is tiny and far below everyday exposure from food, water, and medications.
MSG
•Monosodium glutamate is a flavor enhancer in food.
•Not used in vaccines.
The key principle:
People compare chemical names, not actual biology. Dose, chemistry, route of exposure, and metabolism determine risk.
Or put more bluntly:
Listing scary-sounding chemicals without context is not toxicology. It’s marketing.
The problem isn't the availability of scientific research.
It's the flood of people misinterpreting complex data with zero training and full confidence.
Access to information is no longer the barrier. Understanding it is.
This isn’t “fixing the front door of the NHS.” It’s setting it on fire.
You can’t demand unlimited same-day urgent care AND unlimited routine care with no extra funding, no extra workforce, and crumbling premises.
https://t.co/WXqnpKXwGf
I know many GP teams have been struggling with this. We want to see our patients.
But instead we are having to lose capacity so that politicians can deliver a soundbite.
I am not sure how much more we can take.
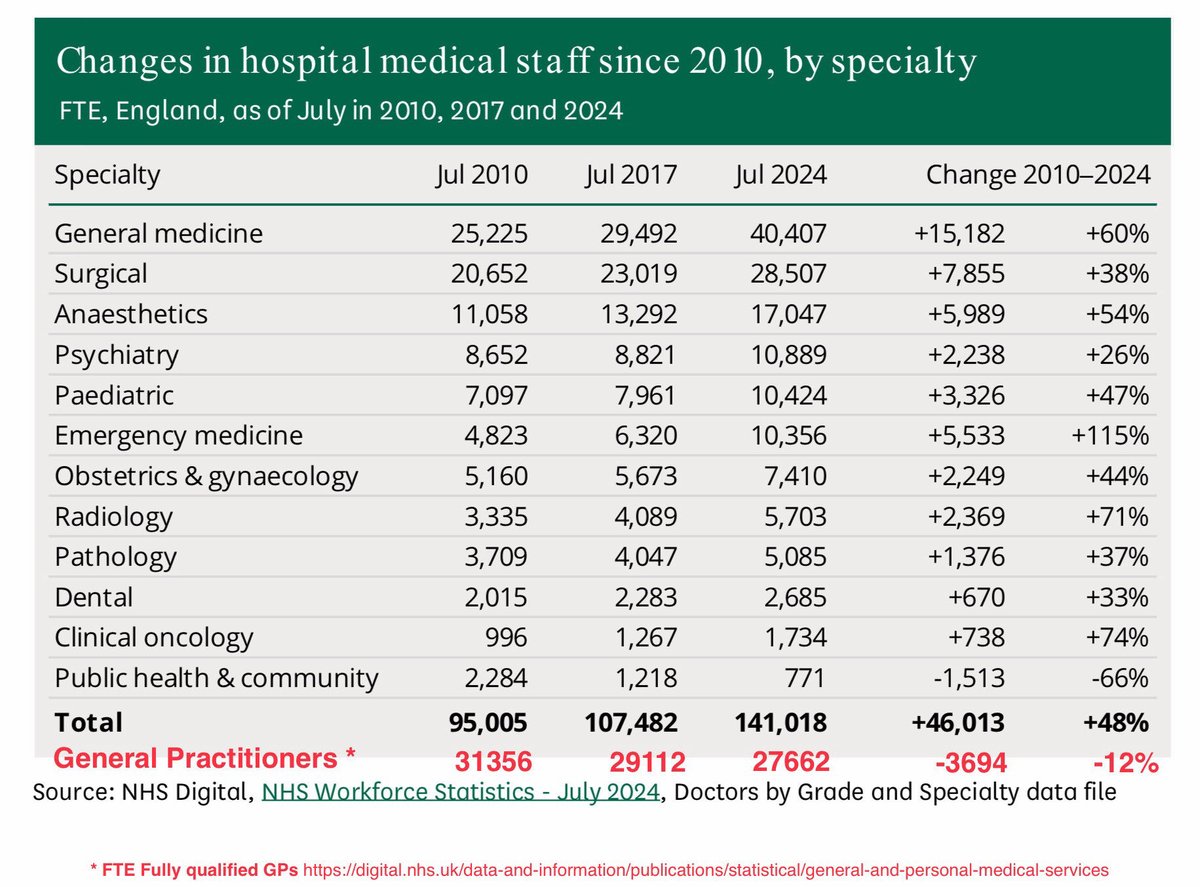
These stats are frankly bonkers. If anybody is complaining about why they are waiting to see a GP. They need to ask why successive governments have not supported the same growth in GP numbers as it has hospital medic numbers
@wesstreeting fix it or fail
Now that everyone is an expert on curing pancreatic cancer in mice, not rats - I want to add some context that goes beyond the headline.
You will want to read this.
Cancer is cured in mice all the time.
Thousands of times. ~90% of those “cures” fail in humans.
Why?
Because mice are:
Genetically simpler.
Treated earlier.
Short-lived.
Not humans.
Mice are a filter - not a finish line.
Yes, this study matters. It comes from the Spanish National Cancer Research Centre.
Yes, it’s pancreatic cancer - one of the deadliest there is. Yes, full tumor regression is impressive.
But here’s what it actually means:
“This approach is now good enough to risk years, trials, and millions of euros on.”
Not:
“Cancer is solved.”
What happens next?
More animal work.
Toxicology.
Phase I (safety).
Phase II (maybe works).
Phase III (beats standard care?).
Maybe 8-10 years if everything goes right.
The real damage isn’t failed drugs.
It’s failed expectations.
Every “cured cancer in mice” headline trains the public to believe:
Cures are being hidden.
Progress should be fast.
Scientists are lying when reality hits.
That’s how trust erodes.
Bottom line:
This is how real cancer progress looks.
Messy. Slow. Risky. Incremental.
Not miracles.
Not conspiracies.
Just science - doing the hard work.
“Statins are toxic and LDL is protective” is not a contrarian insight—it’s the flat-earth theory of cardiology, dressed up with YouTube links and performative skepticism.
LDL (ApoB-containing lipoproteins) is causal in atherosclerotic cardiovascular disease. This is not inferred—it is demonstrated across independent lines of evidence:
• Genetics: familial hypercholesterolemia produces premature atherosclerosis in direct proportion to LDL exposure
• Mendelian randomization: lifelong lower LDL → lifelong lower event rates
• Randomized controlled trials: LDL lowering reduces MI, stroke, and mortality
• Dose–response: more LDL reduction = more risk reduction
• Imaging: LDL lowering leads to plaque stabilization and regression
You do not overturn this with vibes, metaphors, or timestamps.
Statins are among the most studied drugs in medical history. Across dozens of large outcome trials, they reduce heart attacks, strokes, and cardiovascular death. Claims of “toxicity” reliably evaporate the moment hard endpoints are introduced—which explains why endpoints are so carefully avoided.
As for the cited authorities: Nina Teicholz now holds a PhD in nutrition. That fact does not rescue the argument—it makes the persistence of error less excusable. Credentials do not negate randomized evidence, and narrative confidence is not a substitute for outcomes.
Georgia Ede operates outside cardiology and substitutes mechanistic speculation and anecdote for clinical endpoints. If LDL were protective and statins harmful, decades of trials would show it. They do not.
This is the standard con: invoke “Big Pharma,” dismiss randomized trials, elevate anecdotes, and then crown LDL—the particle found inside atherosclerotic plaques—as “protective.”
When someone tells you LDL does not cause heart disease, they are not misunderstood—they are wrong. And when they call statins “toxic,” what they really mean is: I don’t like evidence that contradicts my brand.
Representative evidence (not exhaustive):
– Scandinavian Simvastatin Survival Study (4S)
– Heart Protection Study (HPS)
– Cholesterol Treatment Trialists’ (CTT) meta-analyses
– Ference et al., JAMA / NEJM (Mendelian randomization)
– Nicholls et al., JAMA / Circulation (plaque imaging)
We are living through the rise of anti-expertise.
The idea that knowing more makes you less trustworthy.
Where evidence is optional,
credentials are suspicious,
and confidence beats competence.
That doesn’t empower people.
It makes them easy to manipulate.