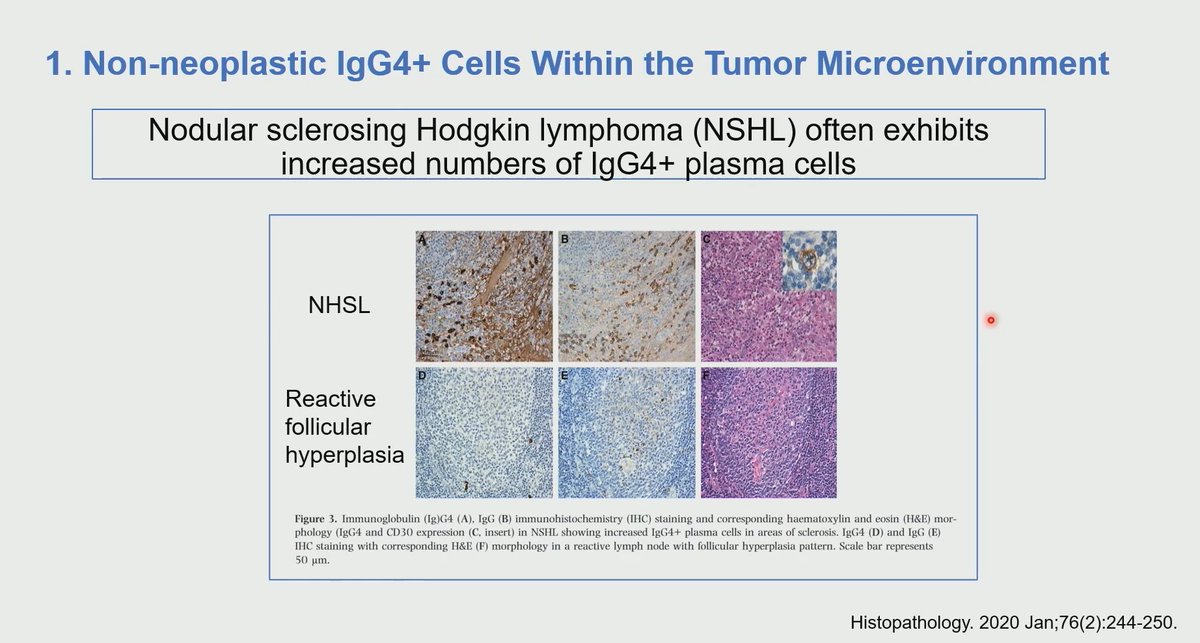
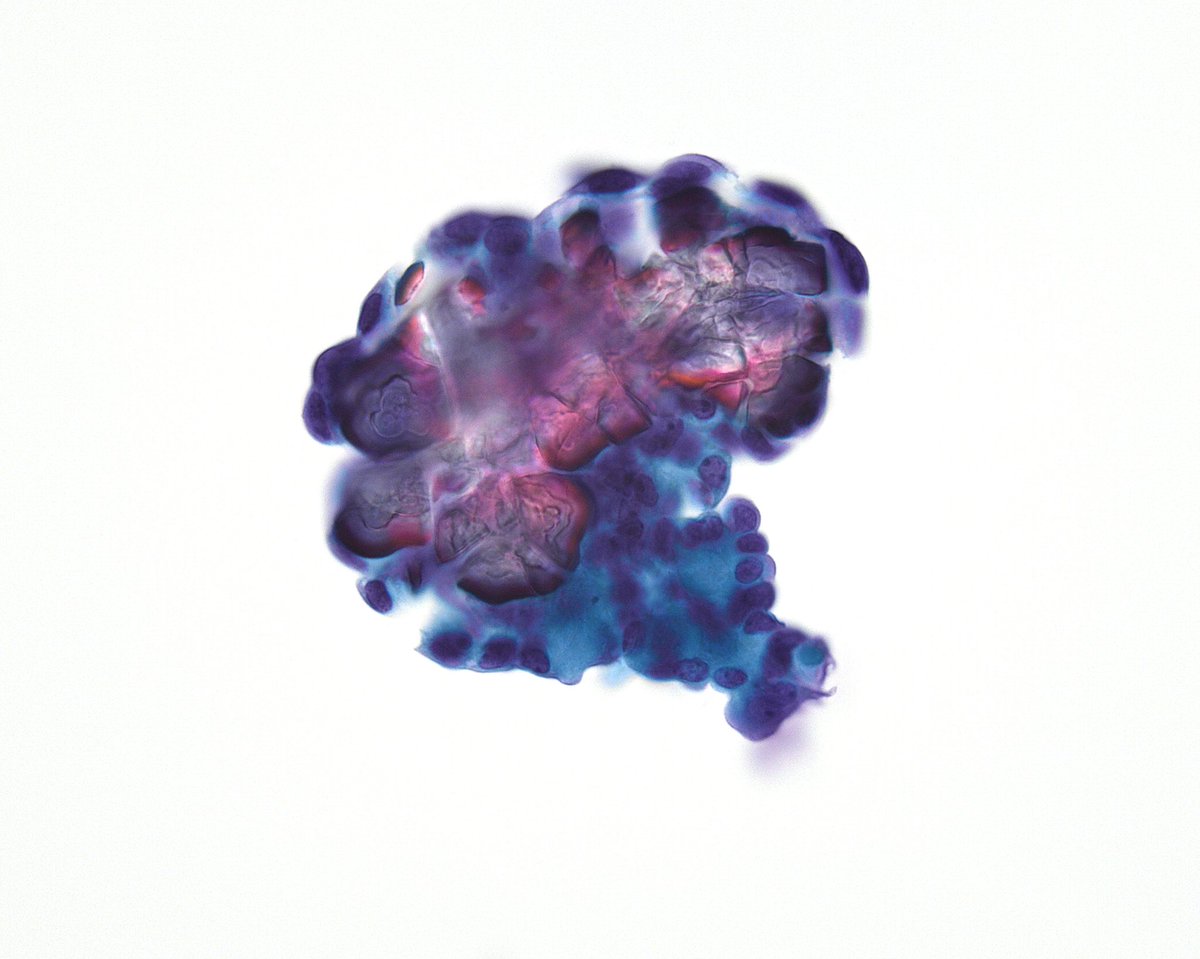
Low-grade B-cell lymphomas may present with prominent reactive inflammatory infiltrates or coexist with autoimmune disorders
⚠️ Increased IgG4:IgG ratio? Stop and think before diagnosing IgG4-related disease. Always exclude an associated lymphoproliferative disorder
What is the cause of abundant IgG4 in lymphomas?Possible explanations...
1. Non-neoplastic IgG4 cells within the tumor microenviroment
2. Monoclonal IgG4 production by lymphoma
3. Lymphoma can coexist with IgG4-related disease and other autoimmune disease
Dr. Herrera Hernandez #USCAP2026 #pathology #PathX #PathTwitter
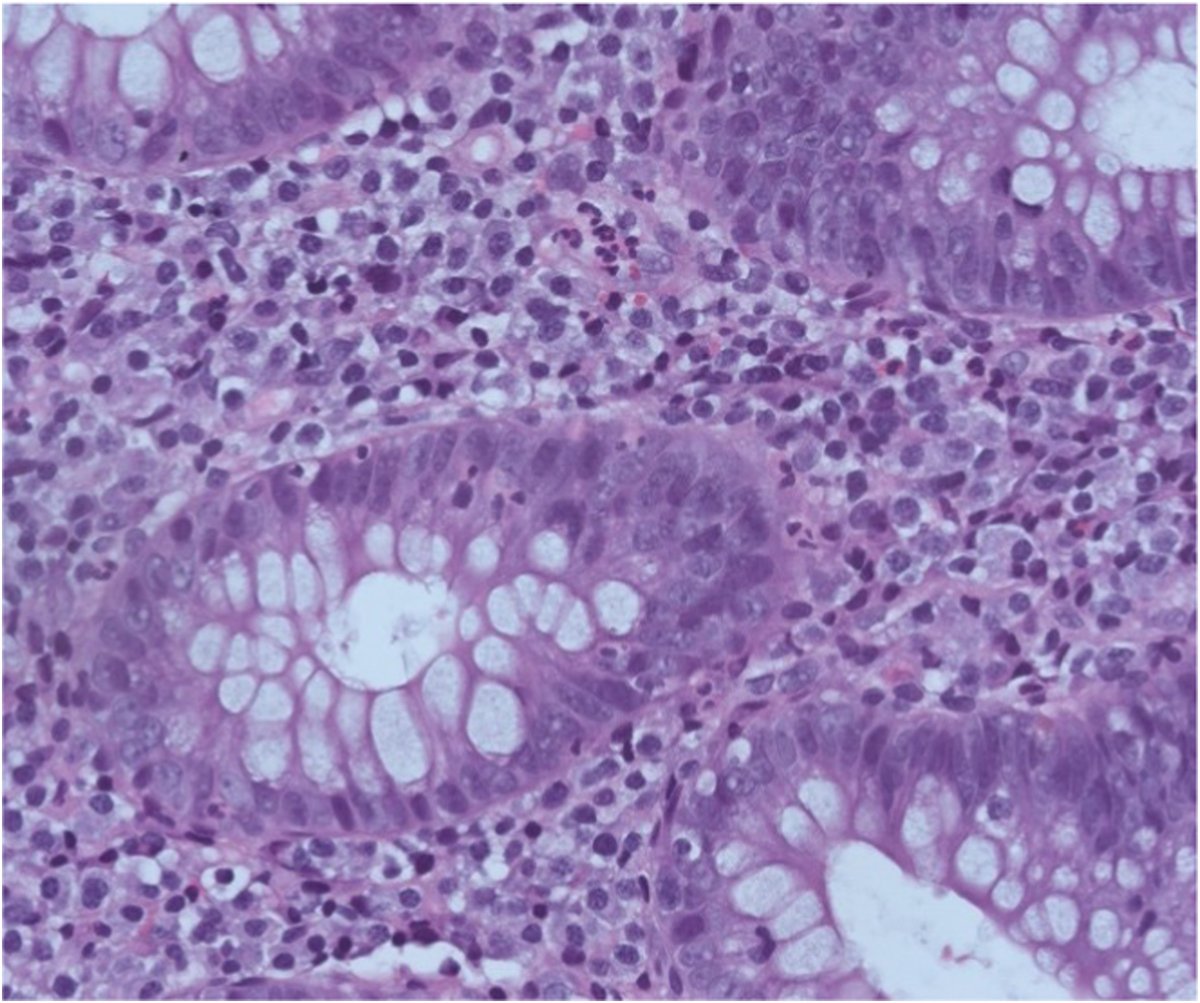
Super excited to share my first post as a publication in @Human_Pathology , Focal active Colitis: Diagnostic Relevance and Long term Clinical outcomes.
Check it out 🙌
Metastatic prostate cancer in skin (it's epidermotropic, meaning dermal metastasis infiltrates epidermis mimicking carcinoma in situ. can cause confusion with skin primary. can happen in melanoma too). Very rare. PSA+. Pics: @SteveBillingsMD#Pathology#dermpath#dermatology
Tumor Deposits in Colorectal Cancer: Definitions for Ninth Edition of the Tumor Node Metastasis Staging System - Modern Pathology https://t.co/VcKALHt3zz
#OpenAccess | Evaluation of 9 antibodies in a set of lung #adenocarcinoma cases, each with 4 matched effusion cell blocks, fixed in formalin, PreservCyt®, CytoLyt® and CytoRich™ Red, respectively.
https://t.co/X2UdSZG85l
@Mansour_cytopat#CytoPath
Revisit the 1st edition of our Cyto-Rads series, which explores the multidisciplinary approach to diagnosing pancreatic pathology and highlights key findings in the most commonly encountered entities in clinical practice.
https://t.co/HzYLjlto10
@MauroSaieg@mdlozanoe@TrieuMD
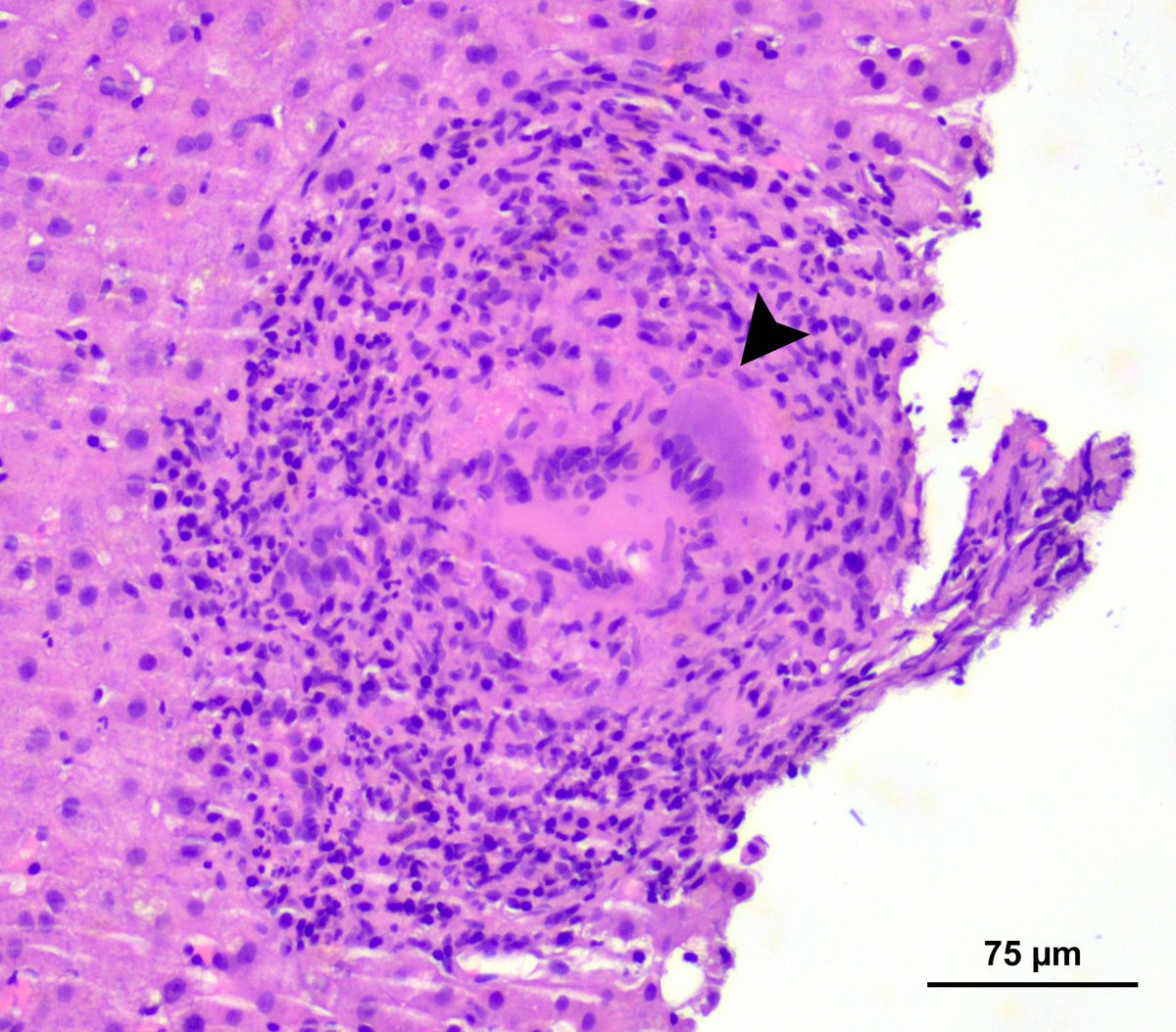
🔬 Hepatic epithelioid granuloma with a multinucleated giant cell (🔼black arrowhead) in BCG-induced granulomatous hepatitis.
💉A rare complication of BCG therapy!
Dr Alessandro Gambella, Pathologist & ESP Alumni, Italy.
#EveryDayPathology#pathology#PathTwitter
“Pen Test” confirming true psammoma body (PB) as opposed to thick colloid (or mucin). Gentle pressure on the cover slip with the tip of a pen while looking at the fragment under the scope will radially fracture a true PB (Thyroid, FNA, PTC). Same fragment, before/after the test.
Practical simple diagnostic algorithm - IHC based for carcinoma of unknown primary.
This is just a simplified algorithm: any suggestions, corrections and additions are welcome
References: 1. Handbook of practical immunohistochemistry; Haiyan Lou
2. Diagnostic
Immunohistochemistry