Consent ✅ - including facial recognition
I have wondered for some time whether a subset of stubborn 'ITB syndrome' cases are actually cases where a distal recurrent branch of the superolateral genicular neurovascular bundle is being compressed under the ITB
This has not been described before
In this case, the patient had bilateral lateral knee pain, which didn't respond to conservative measures, and so underwent partial ITB release - this made him worse
His symptoms now simply on sitting and walking - not just classic downhill running and cycling
Pain is felt diffusely above and below lateral joint line
Previous diagnostic injection around the potential culprit SLGN branch (sat deep to a thickened ITB post surgery in heavy scar tissue) abolished his pain on the treadmill post procedure - but unfortunately no lasting therapeutic effect
So I agreed to step outside of my comfort zone and do something completely novel - radiofrequency ablation (RFA) of this specific nerve bundle under US guidance placement with the help of my pain specialist consultant colleague (see video reel)
NOTE - this is not the well described pain specialist SLGN target up stream at the deep lateral femoral periosteal border (growth plate level) which is often done under fluoroscopic guidance eg for advanced OA knee in patients unsuitable for arthroplasty
During the trochar placement and RF current being applied to the bundle, the patient reported that is was his typical pain
We shall see how his symptoms improve (with the untreated contralateral side as a reference point) over the next few weeks
𝐒𝐭𝐨𝐩 𝐋𝐚𝐛𝐞𝐥𝐥𝐢𝐧𝐠. 𝐒𝐭𝐚𝐫𝐭 𝐑𝐞𝐚𝐬𝐨𝐧���𝐧𝐠.
𝐀 𝐧𝐞𝐰 𝐟𝐫𝐞𝐞 𝐠𝐮𝐢𝐝𝐞 𝐟𝐨𝐫 𝐌𝐒𝐊 𝐩𝐡𝐲𝐬𝐢𝐨𝐭𝐡𝐞𝐫𝐚𝐩𝐢𝐬𝐭𝐬 𝐰𝐡𝐨 𝐚𝐫𝐞 𝐭𝐢𝐫𝐞𝐝 𝐨𝐟 𝐠𝐮𝐞𝐬𝐬𝐢𝐧𝐠 𝐰𝐢𝐭𝐡 𝐩𝐨𝐬𝐭𝐞𝐫𝐢𝐨𝐫 𝐡𝐢𝐩 𝐩𝐚𝐢𝐧.
Your patient points to their buttock. They've already seen someone. They've been told it's their piriformis. Or their SI joint. Or that they need to stretch more.
None of it worked. And now they're sitting in front of you.
Here's the problem: most of us were taught posterior hip pain as a list. SIJ. Gluteal tendinopathy. Deep gluteal syndrome. Proximal hamstring tendinopathy. We match the location to a label and hope for the best.
But posterior hip pain doesn't work like that. Conditions overlap. They coexist. They refer into each other's territory. And a labelling approach — matching a diagnosis to a spot on a diagram — will let you down more often than it helps.
What you actually need isn't a better list. It's a better way of thinking.
What's in the guide
-I've put together a free clinical reasoning framework specifically for posterior hip and buttock pain. It's a PDF you can download, print, and pin up in your clinic.
-It's built around six discriminating questions that help you systematically narrow the differential — not by memorising conditions, but by asking the right things in the right order.
A printable cheat sheet table you can use as a quick-reference during assessments. Imaging guidance on when ultrasound, MRI, or plain film actually adds value.
Link below for Free Download
https://t.co/shJVEwyUNC
You don’t train upper body power & it’s DESTROYING your athletic development
These are 9 variations that will turn your training up a notch
Save this, use them
1. Bilateral band pulses
2. Feed into med ball chest pass
3. Physio ball half moons 🌒
4. Bent over repeat med ball chest pass
5. Prone rapid t raise catches
6. Unilateral physio ball pulses
7. Unilateral band pulses
8. Prone unilateral physio ball pulses
9. Prone battle rope pulses
STOP doing endless cone tap dancing drills and calling it “agility.”
Most athletes are getting worse at actual game speed while thinking they’re training agility
Real agility = reacting to a person/ball + forceful acceleration + deceleration in multiple directions
Save this entire thread
Here are the 6 actual pillars I use to build real, transferable agility with my athletes.
This is the blueprint. 👇
A lot of conversations around stiffness miss the point because they treat it like one quality.
Tendon stiffness and muscle stiffness adapt to different stimuli and both matter if the goal is speed.
Heavy strength work and long duration ISOs expose the tendon to high strain
12/ Summary:
• Olive oil as your main fat
• Handful of nuts daily
• Legumes and vegetables at every meal
• Fish a few times per week
• Minimize processed food and red meat
4,000 years of tradition. 25 years of data. 30% fewer cardiovascular events.
Start with the olive oil.
The hormone no one warned you about:
Insulin
When it’s high, it blocks fat loss, drains your energy, & speeds up aging.
Here are 7 science-backed hacks to lower insulin & finally burn fat:🧵
Consent✅ - this is a beauty 🤓
Elite runner
Crampy, aching lateral knee pain - onset at around 20-30 mins
Seen multiple clinicians - had numerous injections including ITB plus extensive rehabilitation - refractory
Almost 'claudicant' in nature - settles quickly on cessation of exercise - spreads both proximal & distal to lateral joint line
No spinal symptoms & LSp assessment clear
No lateral compartment pathology eg meniscal tear
Had popliteus tendinopathy on US, but minimal response to my initial diagnostic injection
POCUS video -
The inferolateral genicular neurovascular bundle ('pepper pot' structure) is seen compressed under the distal ITB on active knee flexion : terminal extension
Patient localises pain in this area with probe pressure
Injection - hydrodissection (CSI, LA) - fluid seen separating plane just superficial to NV bundle
100% pain relief on extended treadmill test beyond 45 mins 👍
I wonder how many recalcitrant 'ITB' cases are actually neurovascular in aetiology? 🧐
Plan - considering angiography, MR neurography & possible distal ITB release at Gerdy's tubercle if not responsive to injection
Consent ✅
Very interesting knee sports medicine case
Waterpolo player with Ehler-Danlos Syndrome (hypermobility) - bilateral posterolateral knee pain after ramp in training in pool & tournament play
Aggravated by 'egg beater' kick in pool - repetitive knee flexion & rotation - also noted on running
Hard to recreate symptoms in clinic -awareness on deep squat, popliteus stress tests & firm glide of notably lax proximal tibio-fibular joint (PTFJ)
Video (watch entire reel) -
1. MRI L & R knee axial T2 - bilateral small cysts adjacent to posterior PTFJ line & also intimately associated with popliteus tendon sheath
2. US pic - popliteus tendinopathy in hiatus
3. US video 1 - cyst seen clearly close to both PTFJ & popliteus
Both popliteus & PTFJ could be responsible based on MOI - so how can we work it out? 🤔 ➡️
4. US video 2 - by injecting local anaesthetic into the cyst (cheat 'gate-way' into culprit structure) can see injectate pass via 'tail' into the PTFJ rather than into the popliteus sheath
Treadmill test post injection - immediate pain relief - now we have more confidence that its arthrogenic, not tendon driven
Differential diagnosis in Posterior Hip Pain - a joint effort with @TheHipPhysio
Remember pain location will vary and is just one piece of the puzzle in diagnosis!
Jump Training vs. Plyometrics
If you dig into Yuri Verkhoshansky’s original work, he was very specific in how he framed the shock method, “sharp, compulsory muscular tension caused by the kinetic energy of a falling body.”
Over time, as the term spread to the West, the
Basketball isn’t just about speed — it’s about control.
Hard stops, sharp cuts, and controlled landings. Hoopers know it’s not always about how fast but how fast you can stop.
@CowgirlsBball
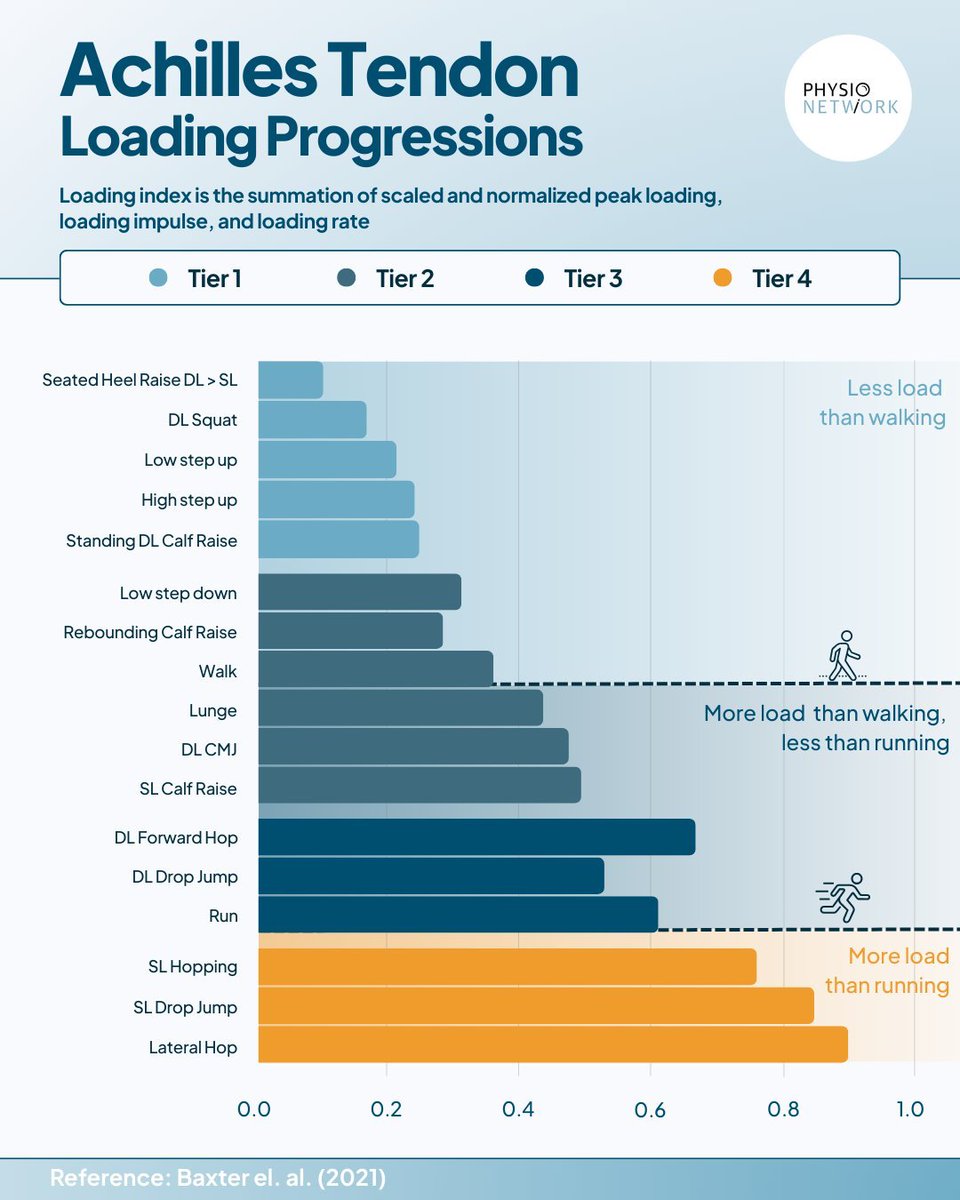
Achilles Tendon Loading Progressions
"Loading index is the summation of scaled & normalized peak loading, loading impluse and loading rate"
@PhysioMeScience@PhysioNetwork@tomgoom
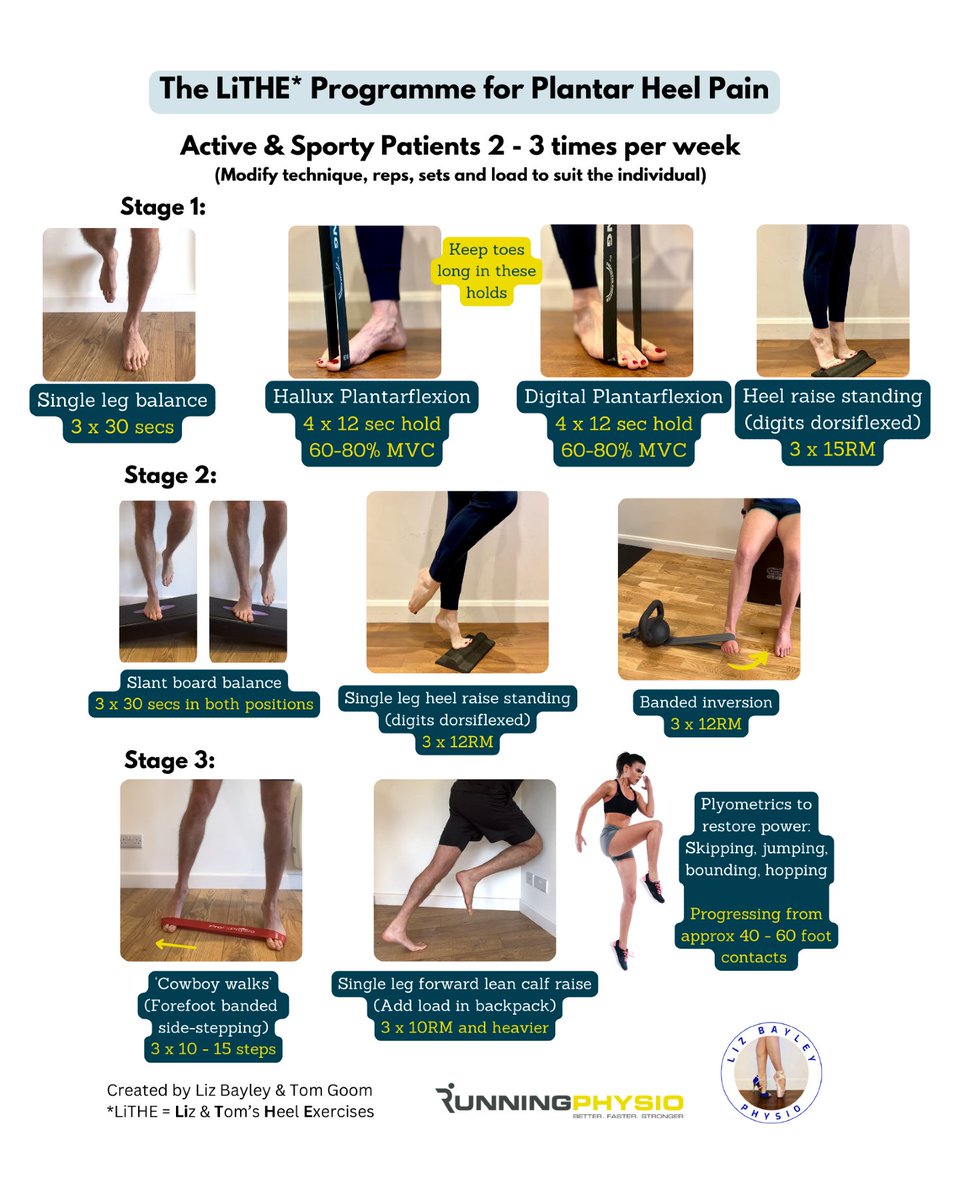
I teamed up with @lizbayleyphysio to create this progressive rehab programme for Plantar Heel Pain.
We've called it 'LiTHE' (Liz and Tom's Heel Exercises) and it's aimed at active and sporty patients. It's not a recipe though so it's best to adapt it to suit individual needs.