$ERAS $ANL
$ERAS were idiots how they played this game. Should not have been dragged into $RVMD scenario and be reactive. Should have waited and released mature data.
But to say that Big Pharma will just give up a $10-15B market and leave it all to $RVMD is ridicules.
Saying "RVMD will get approved first and take the whole market" is plain stupid. Never happened before.
There are many strategies Big Pharma can play with: first line, combinations.....
There is no way, because there is just no way. that this market will be left to $RVMD to play in alone.
And there are only two ways you can play this theme in public markets : $ANL or $ERAS.
All in all I think $ANL is the winner from the late $RVMD - $ERAS debacle.
Also, patent disputes are typically settled in courts. Do you really think big-pharma well just sit on their hands while and let $RVMD have a $9B market (only in PDAC) just for themselves? $ERAS $ANL
$ERAS if PRMT5i combo a hit, what prevents $ERAS from initiating a ph3 trial at the same time as $RVMD? What stops $BMS from picking up $ERAS and competing with $RVMD neck-to-neck? Scratching off all strategic value from $ERAS due to a 2yrs lag is ridiculous.
100% agree. $ERAS got a beating that may have been well deserved given the the bloated valuation and hastened data report, but remains, along with $ANL, the only playable RAS names. $ANL much cheaper and with less of a patent overhang should pickup ahead of data.
Putting criticism about timing and data presentation aside, $ERAS' ERAS-0015 seems very similar to $RVMD's daraxonrasib imo.
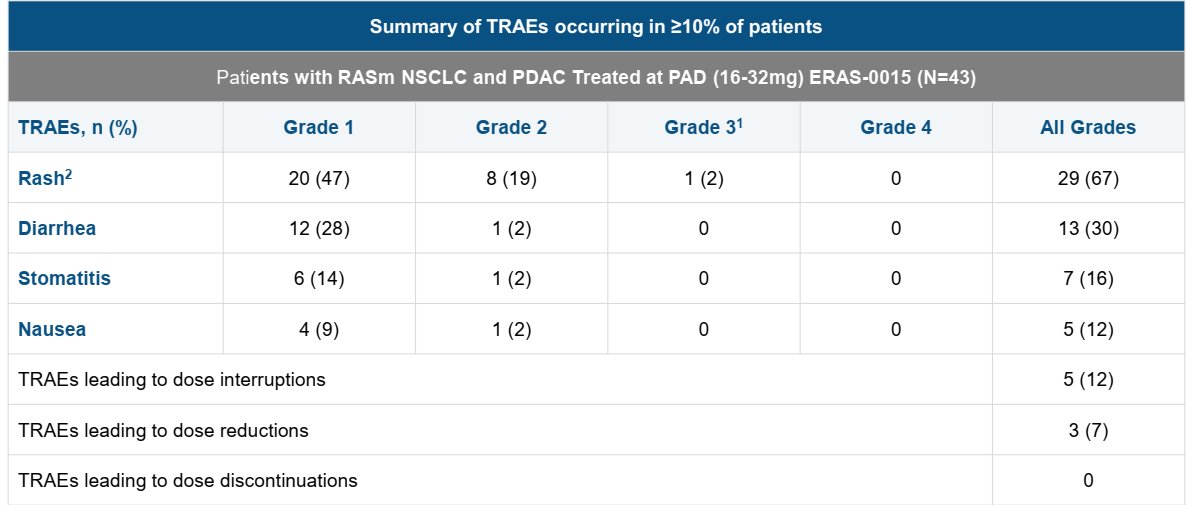
ERAS-0015 is more potent which explains the lower exposure required for efficacy (and associated with on target toxicity of course). It might have a slight advantage on GI side effects (to be seen) but other than that it is likely to have a similar therapeutic index.
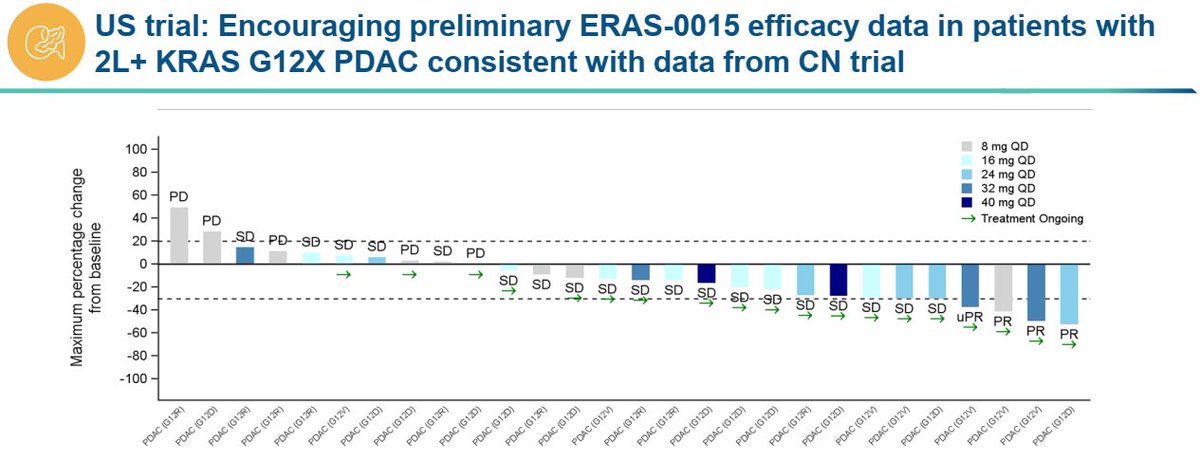
If we compare just the PDAC data sets, $ERAS reported 4 PRs in 21 patients (~19% ORR) in the US at relevant doses which is lower than dara's 35% ORR but that gap will likely close with more follow up as $ERAS has multiple near PRs at the first scan than can convert in the future (They need 3 such conversions to reach 33% ORR).
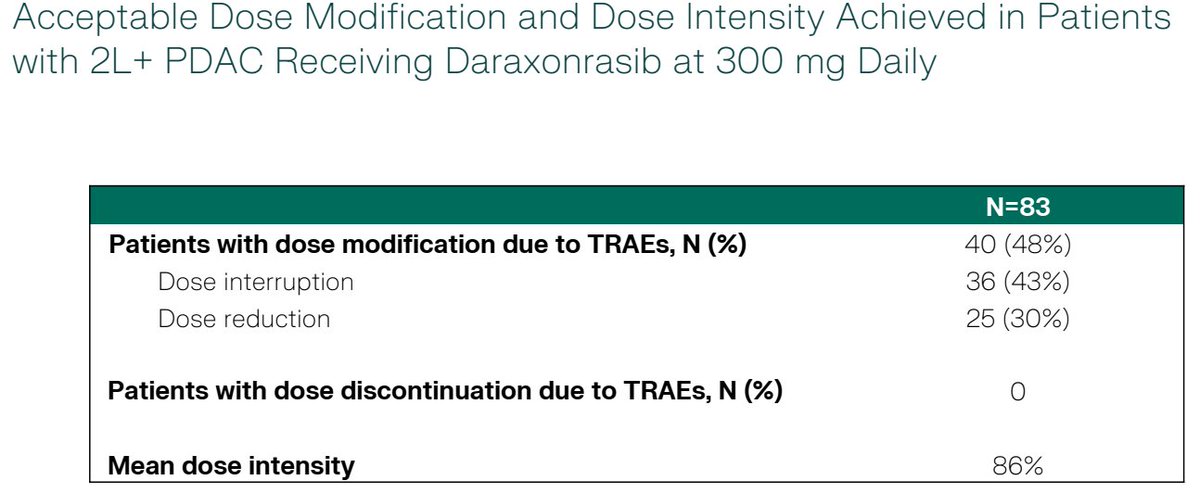
The limited follow up probably has a confounding effect on safety as well (longer treatment typically leads to more side effects) which should take $ERAS to a similar dose interruption/reduction rate in the future. Gr5 pneumonitis case requires attention but it could be an isolated case.
Is $ERAS cheap at $3B? Not sure but for pharmas who cannot afford or simply won't get $RVMD this is the closest fast follower program that could be P3 ready later this year.
*no position in stocks mentioned *
Putting criticism about timing and data presentation aside, $ERAS' ERAS-0015 seems very similar to $RVMD's daraxonrasib imo.
ERAS-0015 is more potent which explains the lower exposure required for efficacy (and associated with on target toxicity of course). It might have a slight advantage on GI side effects (to be seen) but other than that it is likely to have a similar therapeutic index.
If we compare just the PDAC data sets, $ERAS reported 4 PRs in 21 patients (~19% ORR) in the US at relevant doses which is lower than dara's 35% ORR but that gap will likely close with more follow up as $ERAS has multiple near PRs at the first scan than can convert in the future (They need 3 such conversions to reach 33% ORR).
The limited follow up probably has a confounding effect on safety as well (longer treatment typically leads to more side effects) which should take $ERAS to a similar dose interruption/reduction rate in the future. Gr5 pneumonitis case requires attention but it could be an isolated case.
Is $ERAS cheap at $3B? Not sure but for pharmas who cannot afford or simply won't get $RVMD this is the closest fast follower program that could be P3 ready later this year.
*no position in stocks mentioned *
$ERAS re lawsuite, anyone who follows this space closely couldn't be surprised. I view it as an acknowledgement by $RVMD that ERAS is a threat, despite the lag. Re data, I think they have a good molecule on their hands. With RVMD @ $30B, what other way to play RAS? $ERAS $ANL
True, but most likely not a real signal given the context of the disease and history of the patient. Not a big deal IMHO. Overall tolerability profile is actually encouraging $ERAS
have to say
really not a great look to not disclose a death in the PR and only mention it in slides. If there really is no correlation, what's the issue
$ERAS pan-Ras data update this afternoon after market close.
also, $RVMD sent Erasca a letter claiming ERAS-0015 violates certain RevMed patents.
https://t.co/QTmyUhT89n