One thing that keeps coming up when scaling AI agents to production is Semantic Caching. Not the concept - the execution. What do you cache? For how long? What about tool calls, user state, & multi-turn conversations?
Here's how I'd approach it - https://t.co/LOIDjoSYC6
@towards_AI
Most apps show everything at once leading to confusion.🤯
At #FEN2026@booleanhunter will explore adaptive interfaces that shift with real-time context.
Not more UI, smarter UI AI-assisted, context-led, less guesswork
Sign up for free to join👇
https://t.co/yAcPRuvXVW
I was expecting this reply from the IT cell. Who better than akka to do the honours?
1) "The call apparently isn't meant for pansies who can't stand the heat.": Right there. The heat whether physical or metaphorical is something your target audience simply doesn't want at their scale of success. Why would a multimillionaire or a PhD from MIT put up with your physical heat or "suffering builds character" heat arc? They already went through it to reach where they are. What's the incentive here?
2) "It is also not meant for those holding regular jobs there, with the only reason being dollar value. If you come back home, you will fail here. That country does pay mediocrity. Sit there, earn and send the money home."
What's the incentive?
3) "It is meant for exceptionally talented guys who can disrupt the status quo back home and be real changemakers in whatever the firld they are in."
Again, what's the incentive?
Akka, vembu etc act like this is some unsolved brahma rahasya. China has done this thing of attracting talents with multiple talent programs for decades now. Not only did they poach ethnic Chinese, they poached even non-Chinese. When Ukraine war was happening, why couldn't GoI poach Ukrainian scientists? Just declare a few million dollars, guaranteed returns, separate posh accommodations and other perks to those who come and contribute and observe how many people come. But no, you don't want to do the work. You want free service. You never want people to profit for their work. You want for free what they earned through sweat, blood and tears over decades. You don't deserve shit.
I stayed in India for 8 years after graduating. In those 8 years I ran a mildly successful startup, creating 70+ jobs, and a lot of taxes since we were profitable. My Whatsapp inbox from my teaching time is full of thousands of messages of people getting prestigious high paying tech jobs. After that as an engineering leader at various orgs, hired at least 50+ more people. Paid multiple crores of personal income tax as well.
I did more than my fair share of creating employment, creating human capital and contributed enough to pay off my subsidised education (I’ll not deny I got more than good enough education both from school and university, both of which are partly paid for by the government)
In those 8 years, of my closest 10 friends, slowly slowly I found 8 of them now have moved outside India. More than half my college group is outside. And eventually on the balance of things, it really started feeling like I’m getting the short end of the bargain and those others who left were getting a better deal in life.
I had always assured myself that
a) I can always go out whenever I want, I am here by choice
b) I’ve consciously stuck to faster growth roles orgs but if I ever wanted to, I can go to big tech too
Finally a switch clicked in the head saying if you’re so sure of (a) and (b) why don’t you really just go and see. You can always come back.
In the long run I might be proven wrong (I’m aware of stories of one health scare or racism incident or ailing parents that pushes the pendulum back for many), but for now my lived experience only taught me exactly opposite of what Vembu has said below. In fact if 10 years ago I would have even slightly been convinced by the below tweet, today I’m convinced even less by it. From my perspective of the things I sought in life, the equation has only gotten worse not better.
@ManaevLab That's interesting! Do you use the string from the last 3 turns as it is, or do you rephrase them into a single self-contained one before using as cache key?
One thing that keeps coming up when scaling AI agents to production is Semantic Caching. Not the concept - the execution. What do you cache? For how long? What about tool calls, user state, & multi-turn conversations?
Here's how I'd approach it - https://t.co/LOIDjoSYC6
@towards_AI
@celebrimbor91 Curious what you mean by replay logs - are you storing the agent's tool call sequence and replaying it on a miss rather than hitting the LLM?
“Not all alcoholic beverages are metabolically or chemically equivalent, and they may have distinct biological effects that could influence health outcomes differently”
Why different drinks produce different effects?
While the ethanol (alcohol) is identical, the delivery system varies.
[1] Alcohol by volume (ABV) and speed of consumption is the most significant factor. Spirits (like vodka or whiskey) typically have an ABV of 40% or higher, whereas beer is around 4-6% and wine is 12-15%. Consuming high-ABV drinks leads to a faster spike in blood alcohol concentration (BAC), especially if taken as shots. A rapid rise in BAC heavily impairs motor skills and judgment much quicker than slowly sipping a beer (doesnt mean sipping beer slowly is useful - any amount of alcohol increases risk of different types of cancers).
[2] Congeners are biologically active chemical byproducts of the fermentation and aging process, including methanol, acetone, and tannins. Darker drinks (bourbon, red wine, dark rum, tequila) have much higher concentrations of congeners than clear drinks (vodka, gin). The body struggles to break down congeners (particularly methanol, which breaks down into formaldehyde and formic acid). High congener levels are scientifically linked to more severe, prolonged hangovers and increased inflammatory responses.
[3] Carbonation or the presence of carbon dioxide, whether in champagne, sparkling wine, beer, or liquor mixed with soda, increases the pressure in the stomach. Carbonation accelerate gastric emptying, the rate at which stomach contents are delivered to the small intestine, where the vast majority of ethanol absorption occurs due to the enormous surface area. Ridout et al. (2003) study in the British Medical Journal, showed that carbonated champagne produced higher early blood alcohol concentrations compared to flat (degassed) champagne at equivalent ethanol doses. The effect was modest and most pronounced in the first 20–30 minutes. Therefore, carbonated drinks lead to a quicker intoxication.
[4] Sweet liqueurs, cocktails, or mixing spirits with sugary sodas can mask the taste of alcohol, often leading to faster consumption. Additionally, high sugar intake combined with alcohol can cause a rapid spike and subsequent crash in blood sugar levels, contributing to lethargy and increasing hangover symptoms. Alternatively, mixing alcohol with diet sodas (which lack sugar to slow gastric emptying) can actually cause the alcohol to be absorbed into the bloodstream faster than regular sodas.
The bottom line from an evidence-based standpoint is that the type of alcoholic beverage is far less important than the quantity and pattern of ethanol consumption. The concept that wine is "healthier" or that certain spirits are "cleaner" has no robust mechanistic or epidemiological support when ethanol dose is held constant.
So do not drink alcohol. It benefits only the manufacturer and the governments who tax it. For you, its your health that is slowly eroding away, one drink at a time.
Good morning @dr_sivaranjani
The Public Interest notice put on social media by Kenvue, the makers of Fake ORS™ is a classical case study in "Corporate Health-Washing".
Hey @kenvue@JNJNews no one needs your rubbish "hydration products" from a scientific standpoint. So you can go to hell and your products can rot on the shelves for all we care. Stop intimidating physicians and clean up your corporate mess born out of greed. Presenting your products in medical conferences is not scientific evidence, its paid endorsement. So respectfully, F.O.
A product that was commercially marketed as ORS for years despite not meeting WHO composition standards, that was formally banned by India's food safety regulator, that had its ban upheld by the Delhi High Court as a "health hazard," and that has now been cosmetically rebranded with a visually similar name, is being presented as a triumph of science-backed innovation. The WHO's own recommendation against the very sweetener used in the reformulated product is dismissed as "unrelated." And the physicians who fought for eight years to protect children from this deception are characterized as "disparaging influencers."
Here is a takedown of their sh*tty notice from my side, which you (@dr_sivaranjani) can use in your case against them.
1. "We have shaped the hydration category in India providing consumers with scientifically formulated solutions"
This is corporate euphemism for having commercialized a high-sugar beverage that was deceptively branded to resemble WHO-standard ORS for years. The product ORSL was never WHO-compliant ORS. The WHO reduced-osmolarity ORS formula specifies glucose 75 mmol/L (~13.5 g/L), sodium 75 mEq/L, potassium 20 mEq/L, and a total osmolarity of 245 mOsm/L. A product with roughly 8–9 times the glucose concentration of WHO ORS is not a "scientifically formulated solution", it is a sugary beverage that can worsen diarrheal dehydration through osmotic diarrhea. FSSAI found that the labeling and branding of ORSL beverages may mislead consumers into believing the product was a medically approved oral rehydration solution.
2. "In January 2026, we diversified our portfolio into two distinct brands — ORSL (Drug product) and ERZL (Food Product)"
This "dual-brand strategy" was not voluntary innovation — it was forced by the FSSAI ban. ORSL has even rebranded to ERZL (the 'e' designed to look similar to 'o' and the 'z' to 's'). The visual similarity between "ERZL" and "ORSL" is not accidental. The product's communication and positioning may create an association with ORS, and references to similarly named products in branding or advertising could reinforce consumer recall and blur the distinction between scientifically approved ORS and commercially marketed electrolyte beverages. A parent who was buying ORSL thinking it was ORS will now see ERZL in the same pharmacy shelf with near-identical packaging and make the same error. This is classic brand continuity engineering designed to circumvent regulatory intent.
3. "Reduced the added sugar content by 87% with 1.4X more electrolytes" — framed as a public health achievement
If you reduce sugar by 87% from a baseline of ~110 g/L added sugar, you still have approximately 14 g/L added sugar - and you have now replaced that sugar with sucralose, an artificial sweetener. The framing of "87% reduction" is a mathematical trick: it sounds impressive only because the starting point was absurdly, irresponsibly high. It is like a tobacco company boasting of reducing tar by 87% and expecting public health applause. Furthermore, "1.4X more electrolytes" is vague and scientifically meaningless without specifying which electrolytes, at what concentrations, and whether the resulting osmolarity is appropriate for the claimed indication. An electrolyte drink for "everyday hydration" in a healthy individual is, physiologically speaking, unnecessary - plain water and a normal diet provide adequate electrolytes for non-pathological states.
4. "There is well established scientific and safety assessment of sucralose, which is recognized by Global Health Authorities like Codex, EFSA besides both FSSAI & CDSCO/Indian Pharmacopoeia"
This statement cherry-picks regulatory approvals while deliberately ignoring the WHO's own 2023 guideline where especially, this ingredient is not supposed to be part of "healthy hydration."
5. "WHO Guidelines (2023) regarding use of 'non-sugar sweeteners' to reduce the risk of unhealthy weight gain have also been cited out of context and is unrelated to products like WHO ORS and Electrolyte Drinks"
This is perhaps the most egregious misrepresentation in the entire notice. The WHO 2023 guideline on NSS is a public health recommendation against the use of non-sugar sweeteners in foods and beverages across the board. This guideline provides evidence-informed guidance on the use of non-sugar sweeteners in adults and children. The guideline explicitly applies to "all synthetic and naturally occurring or modified non-nutritive sweeteners found in manufactured foods and beverages." ERZL is a manufactured beverage containing sucralose. It falls squarely within the scope of this recommendation. Kenvue's argument that this guideline is "unrelated" to electrolyte drinks is scientifically untenable. The WHO did not carve out exceptions for beverages that happen to contain electrolytes. The guideline's scope is defined by the presence of NSS in the product, not by the product's marketing category.
6. "We have been singularly targeted by a few Healthcare Professionals cum influencers in a disparaging and denigrating manner"
The healthcare professionals who raised these concerns were exercising their professional duty. Dr. Sivaranjani documented cases over eight years, including a diabetic child from Chennai who was dehydrated despite being given an ORS drink from a tetra pack. It was her advocacy that ultimately led FSSAI to act.
Characterizing physician advocacy against misleading health products as "disparagement" is a well-documented corporate strategy (SLAPP: Strategic Lawsuit Against Public Participation) designed to silence public health criticism through legal intimidation.
The notice's claim that these professionals are motivated by "commercial benefits" and "increasing followers" is an ad hominem attack that inverts the actual conflict of interest. The commercial benefit accusation is outrageous - the party actually benefitting commercially from the product is the company Kenvue (Johnson & Johnson).
7. "We always recommend our ORSL WHO ORS portfolio to address diarrheal dehydration and ERZL for everyday hydration, respectively"
The concept of "everyday hydration" requiring a commercial electrolyte-and-sucralose beverage has no basis in physiology or evidence-based medicine. It is not recommended in any clinical guidelines. Healthy individuals with intact renal function, normal diet, and access to water do not need electrolyte supplementation for everyday activities. "Silent dehydration" - a marketing term promoted by these manufacturers - does not appear in recognized medical literature. This framing medicalizes a normal physiological state to create a market for an unnecessary product.
8. "We had no choice but to take necessary action to safeguard the brand integrity"
Sending legal notices to physicians who raise legitimate scientific concerns about a product that was already banned by FSSAI and whose ban was upheld by the Delhi High Court is not "safeguarding brand integrity." It is an attempt to suppress public health advocacy. The timing - sending notices after being forced to rebrand by regulatory action - suggests the motive is to silence documentation of the rebranding's deceptive visual similarity to the original banned product, not to correct misinformation.
The science is not on Kenvue's side. The regulatory record is not on Kenvue's side. The public interest is not on Kenvue's side.
This is an Orwellian nightmare. Basically he is saying that the state will now photograph your car and debit your bank account directly. No court order, no notice, no consent, no due process. Just a camera, an algorithm, and instant access to your money. And millions of people will clap for this because muh "technology" and "no more queues."
Every wrongful deduction, every misread plate, every system error will drain your money first and maybe, if you're lucky, get reversed months later after you run around in circles with government authorities and court cases. But alas, those of us who call this out will be labelled aunty nashnul luddites.
Standing up for accurate medical information should never invite intimidation. Absolutely. I applaud Dr. Sivaranjini for her fight against misleading ORS branding, and every doctor who rallied behind her. This is what the medical community should look like.
But let me be honest. Painfully honest.
The medical community in India develops courage selectively - when the stakes are low and the enemy is convenient.
Fighting fake ORS is important. But it is also safe. No ancient tradition protects it. No ministry backs it. No political ideology wraps itself around electrolyte branding.
Now try standing up against Ayurveda and Homeopathy causing liver failure, kidney injury, lead poisoning, and death. Try publishing that data. Try saying it out loud on a public platform.
I have been doing this for years. What has it earned me? Fifteen-plus legal notices. Criminal cases. FIRs. Defamation suits filed across multiple states. Harassment, bullying, and coordinated attacks from an industry that enjoys state protection and cultural immunity.
And where has the medical community been?
Largely silent. Comfortably silent.
By-and-large, the medical community especially the medical student community, the specialists clinical societies or national and regional level doctors group never come out and fought for the rights of the patients and their safety against Ayush in India in the open - not even endorsing evidence after evidence of harms published.
The gastroenterology and hepatology societies in India - my own specialty - do not hold sessions on alternative medicine at their national meetings. They do not publish guidance for patients. They reject manuscripts documenting AYUSH adverse events. Their consensus statements pretend the problem does not exist. They have decided that this particular cancer growing inside Indian public health is someone else's problem.
For years, the medical establishment believed that if they ignored AYUSH harms, if they simply didn't talk about it, the problem would disappear. It didn't. It metastasized. And now have infiltrated Institutions of repute. And while it grew, the people who stood by me, who amplified the evidence, who fought alongside me — were not doctors. They were not specialist societies. They were not medical colleges.
They were the public. Ordinary citizens who understood that patient safety is not a niche academic concern - it is their lives, their families, their right. And I want them to know, that I appreciate you. You are my sanctuary here.
I love what I do. I have no complaints. I will keep doing it as long as I can. But imagine, just imagine, what we could have achieved if the entire medical community had treated AYUSH harms with the same urgency they now show for fake ORS. If every clinical society had said: our patients are being poisoned by unregulated products sold as medicine, and we will not stay quiet.
We would have had better regulation. Better research. Better outcomes. Fewer destroyed organs. Fewer dead patients. Fewer transplants.
"Death is the sound of distant thunder at a picnic."
That is what AYUSH toxicity is to the Indian medical establishment - a distant rumble they can ignore while they enjoy their conferences. Until the storm arrives at their own table.
It shouldn't take one doctor being dragged to court for the community to notice. It shouldn't take a patient dying for a society to issue a statement. Stand up for all of patient safety. Not just the parts that don't cost you anything.
Dismantle the narrative Ayush is building. This is, the only beast, medical community in India must handle effectively to improve healthcare outcomes and public and patient safety.
VERY IMPORTANT ANNOUNCEMENT.
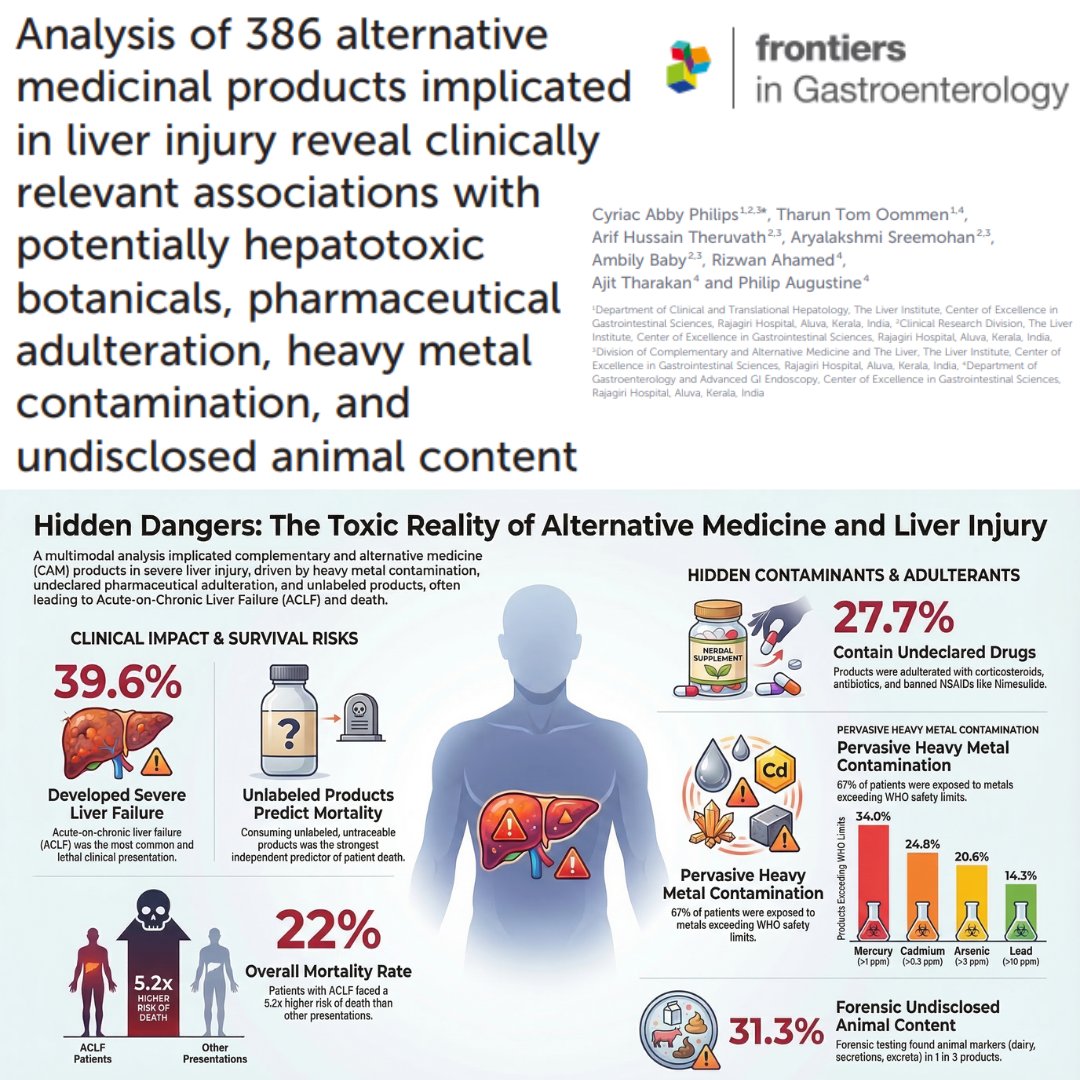
Dear friends, we have published the largest analytical study of Ayurveda, Homeopathy, Siddha, Unani and Folk-Traditional Medicinal products that have harmed patients - presenting with liver damage - to our department. This is the most exhaustive analytical study that correlated clinical outcomes in such patients.
Interestingly, one of the Reviewers who peer-reviewed our paper (notification after paper publication) and cleared it for publication is a senior professor of Ayurveda (Rasashastra and Bhaishajya Kalpana) at All India Institute of Ayurveda. This makes our paper even more impactful.
Here is a plain language summary of the study's major findings, highlighting what patients and the public need to know about the safety of alternative medicines:
Severe Liver Damage is a Major Risk: The study looked at 386 alternative and complementary medicines taken by patients who experienced liver damage. It found that these products frequently triggered a severe, life-threatening form of liver failure, called Acute-on-chronic liver failure (or ACLF) which resulted in death for nearly 40% of the patients who developed it.
Unlabeled Products Can Be Deadly: Taking "unlabeled" products—those sold without proper ingredient lists, manufacturer details, or batch numbers—was a strong predictor of death. The risk of dying increased the more unlabeled products a patient consumed, showing how dangerous an unregulated supply chain can be. Data revealed a dose-response relationship where death rates escalated progressively, reaching 42.9% among patients who consumed three or more unlabeled products.
Dangerous Levels of Heavy Metals: A shocking number of the tested products were heavily contaminated with toxic metals like mercury, lead, arsenic, and cadmium, often at levels far above safety limits. Exposure to cadmium, in particular, was strongly linked to patients developing the most severe form of liver failure. Exposure to cadmium was strongly and significantly associated with the development of ACLF (75.9% in exposed versus 22.6% in unexposed patients).
Hidden Prescription Drugs: Almost one-third of the products secretly contained modern pharmaceutical drugs, meaning patients were taking them without knowing. These hidden drugs included steroids, antibiotics, and painkillers, and some were even banned or well-known to cause liver damage.
"Natural" Doesn't Always Mean Safe: Over 40% of the products contained plant ingredients that are medically documented to be toxic to the liver. Well-known herbs like Giloy (Tinospora cordifolia) and Ashwagandha were among the most common potentially harmful plants found in the products.
Secret Animal Ingredients: Testing revealed that nearly a third of the products contained undisclosed animal ingredients (such as dairy, marine products, or animal extracts). This is a major concern for vegans, vegetarians, and people with religious dietary restrictions who believe they are taking plant-based medicines.
Risks from Concentrated Plant Extracts: The study discovered that high concentrations of certain common plant fats and compounds (called phytosterols) were tied to higher rates of severe liver failure. This shows that highly concentrated "natural" extracts can act differently in the body and become harmful, even if they come from everyday plants.
Lead Reseacher: @arifhussaintm
FULL PAPER (free to read): https://t.co/3RIqoZdXyD
Good morning. Felt like treating this delusion right away.
This is a textbook case of "retroactive pattern-matching" which is the (dumb) intellectual equivalent of firing arrows at a wall and then painting bullseyes around them.
This is a special category of mental health disorder Indian social media sympathizing with pseudoscientific Ayurveda suffers from - The "We Knew It First" Syndrome.
Claim 1 - "Ayurveda described atherosclerosis thousands of years ago as Dhamani Pratichaya"
In the Ayurvedic classical text, Charaka Samhita, Sutrasthana Chapter 20, Dhamani Pratichaya ("hardening of vessels") appears as an item in a list of 20 diseases attributed to "kapha dosha" imbalance.
Kapha Dosha is an imaginary energetic bodily fluid - among Kapha, Pitta and Vata humoral theory which became obsolete in late 18th century.
Ayurveda also claimed the mind is inside the heart.
Observing that arteries get blocked is not a discovery. Ancient Egyptians documented atherosclerosis in mummies as well as Greeks too. Noticing that fat accumulates in vessels is about as revolutionary as noticing that drains get clogged.
Claim 2 - "PLTP enzyme = Lekhana (scraping) principle"
This is where the claim goes from wrong to comical. PLTP is a specific ~81 kDa glycoprotein that transfers phospholipids between lipoproteins, facilitates cholesterol efflux to HDL via ABCA1-mediated pathways, and operates through precise protein-lipid interactions at the molecular level involving apoA-I-containing lipoproteins. Calling this "Lekhana" (scraping) is like saying ancient people invented aviation because they observed birds flying.
Claim 3 - "Guggulu is the ancient world's PLTP"
This is the crown jewel of the delusion, and the evidence here is deliciously ironic.
The landmark JAMA 2003 randomized controlled trial tested standardized guggul extract in adults with hyperlipidemia.
The result?
Compared with placebo participants in whom LDL-C decreased by 5%, both standard-dose and high-dose guggulipid actually raised LDL-C by 4–5%, for a net worsening of 9–10%. There were no significant changes in total cholesterol, HDL-C, triglycerides, or VLDL-C. Six participants also developed hypersensitivity rashes from guggulu. So Guggulu is the ancient world's delusionally harmful PLTP. https://t.co/jTyynfxRIE
Wait. It does not end there.
A later RCT combining guggulu with Triphala (another Ayurvedic BS) showed equally dismal results: three months of treatment showed no better effects than placebo on serum levels of total and LDL cholesterol, BMI, or waist circumference: https://t.co/UK7IvwaIZA
A Natural Standard Research Collaboration review concluded bluntly: there is not enough scientific evidence to support the use of guggul for any medical condition: https://t.co/FesrhtTteM
But wait once more. Here's the part that should concern everyone: guggul and its bioactive compounds have been implicated in possible and probable drug-induced liver injury with a severe liver damage, and there have been reports of acute liver failure requiring liver transplantation: https://t.co/nqLUP7Irzx
In summary, what's happening here is a well-known rhetorical trick: take a vague ancient description, wait for modern science to discover something specific, then retroactively claim the vague description was "the same thing." This works because vague claims can be mapped onto almost anything.
More examples:
"Ancient texts described channels in the body" → Therefore they knew about ion channels!
"Ancient texts said food gives energy" → Therefore they knew about mitochondrial oxidative phosphorylation!
"Ancient texts said the sky has lights" → Therefore they knew about nuclear fusion in stellar cores!
If you "scrape" the base of the skull of these types of people on social media, you will only find guggulu molecules, not neurons.
One irony I’ve noticed in certain younger crowds, (especially among certain yoga/spirituality–adjacent circles, functional medicine types, etc.): is how hyper-optimized they get about tiny insignificant health variables. If you have a piece of chocolate in front of them, they will shake their head in disapproval & say "oooh sugar is poison 😱" & will try to micromanage every ingredient & throw around buzzwords like 'gut microbiome', 'natural immunity', 'microplastics', 'inflammation' etc obsessing over marginal gains.
Yet those same people will also smoke a cigarette or a joint in a day, or have no problem with drinking alcohol once a week or so - substances that are either established Group 1 carcinogens or at least far less studied. If you then question them, suddenly the philosophy shifts to 'everything in moderation' or 'you have to live a little'.
Like… bro c'mon make it make sense 😂. You find "toxins” in seed oils & gluten but not in literal smoke? 😂 . Pick a philosophy and be consistent, no?
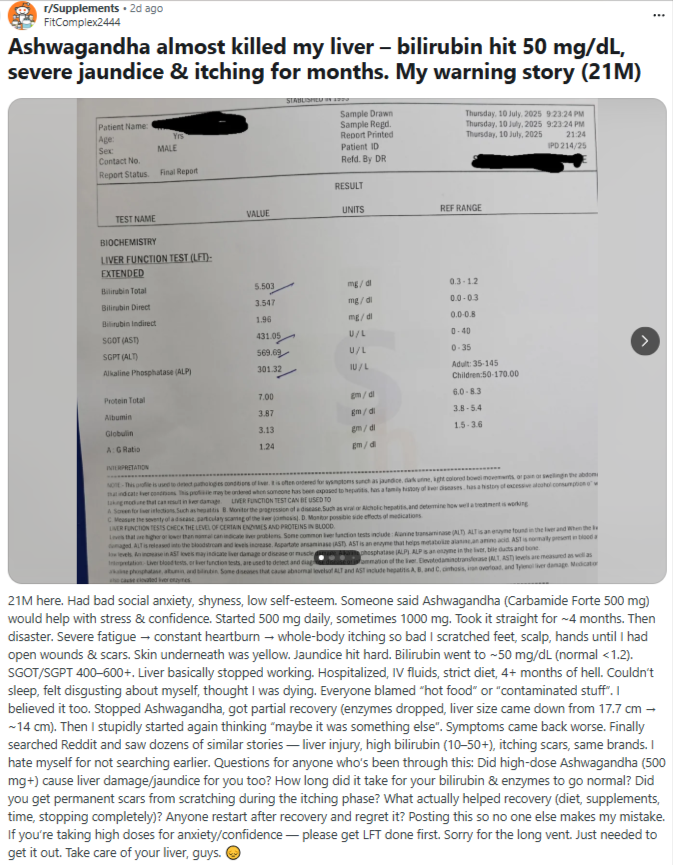
Ashwagandha is heavily promoted on social media by fitness influencers and gym enthusiasts as a wonder supplement, but the science behind its claimed benefits is surprisingly weak.
The few clinical trials that exist are small, poorly designed, and often funded by the supplement industry itself, making the results unreliable.
What is much better documented, is that Ashwagandha can harm the liver. The US Drug-Induced Liver Injury Network now lists Ashwagandha as one of the top herbal products causing liver damage.
The largest case series from India (by me and my colleagues) showed that Ashwagandha caused serious liver injury on its own, without any contamination or adulteration, and in people who already had liver problems, it triggered liver failure and death.
Several other cases worldwide have needed emergency treatment including plasma exchange, and some have been evaluated for liver transplantation.
Ashwagandha continues to be popular despite having no solid proof of benefit and no proper safety data — making it a preventable cause of liver disease fueled by marketing, not medicine.
Buyer, beware.
@theliverdoc Sad thing is, it's not just nutritionists, but also lot of personal trainers in the gym are advising their clients to take supplements beyond whey protein (like ashwagandha, ginseng extract, green tea extract etc).
@IanCopeland5 To all the idiots supporting these parents, this is what you sound like: “You’re lying pieces of shit about this medical science you’ve developed to prevent a lung illness, but I trust you completely about the medical science you’ve developed to transplant lungs!”
This is a recycled myth built from misreading observational geriatric data, and it collapses once you apply basic epidemiology and clinical trial evidence.
1. Japan’s longevity does not come from high cholesterol
Yes, Japan has high life expectancy.
No, that is not because elderly Japanese have high LDL.
Japan’s outcomes track with:
Low lifetime LDL exposure (dietary pattern, not late-life labs)
Low obesity
Low smoking in women
High physical activity
Strong social cohesion
Universal healthcare
Late-life cholesterol snapshots do not represent lifetime exposure, which drives atherosclerosis.
2. “High cholesterol = longer life in the elderly” is reverse causation
This is the key error.
In older adults:
Low cholesterol often reflects frailty, malnutrition, cancer, inflammation, or chronic disease
People already sick tend to have lower cholesterol and higher mortality
That does not mean cholesterol is protective.
It means illness lowers cholesterol.
This is called reverse causation, and it is a first-year epidemiology concept.
3. Observational studies ≠ treatment decisions
Those studies:
Are non-randomized
Do not test statins
Do not measure lifetime LDL burden
Do not show benefit from raising cholesterol
They describe who is already dying, not what prevents disease.
4. Statins in older adults: what the evidence actually shows
Randomized controlled trials and meta-analyses show:
Statins reduce heart attacks and strokes in older adults
Benefits persist into the 70s and early 80s
Absolute benefit is often greater because baseline risk is higher
Side effects:
Muscle symptoms occur in a minority and are usually reversible
No consistent evidence of cognitive harm
Statins reduce dementia risk overall in large population studies
The “statins rot grandma’s brain” claim is simply false.
5. The 230 cholesterol scare story is a straw man
No competent physician treats a number in isolation.
Decisions are based on:
Overall ASCVD risk
Prior heart disease or stroke
Diabetes, blood pressure, smoking
Functional status and goals of care
Frailty, limited life expectancy, or intolerance → don’t treat
High risk, good function → treat
That’s medicine, not profit.
6. “Follow the money” fails reality
Statins are generic, cheap, and off-patent
They save health systems money by preventing expensive hospitalizations
If profit were the motive, cardiology would push far pricier drugs first
(they don’t)
Bottom line
High cholesterol in the elderly is not protective
Low cholesterol in sick elders reflects underlying illness
Lifetime LDL exposure still drives atherosclerosis
Statins help selected older adults live longer and better
This argument confuses survivorship bias with science
This isn’t “protecting grandma.”
It’s misusing statistics to scare families away from evidence-based care.