“Patients need doctors and doctors need jobs”
Today, we've written to @wesstreeting to ask the Government to resume talks – and work with us to agree a viable deal on pay and jobs.
Without movement on both, we’ll be left with no choice but to return to the picket lines.
@TheKingofBen @DrEilidhMaria@CareQualityComm I wouldn't ignore it, but any concerns may be better directed to the event medical company directly if the name of the company is known, and/or the event organiser, because the CQC simply may not have a remit to be involved.
@TheKingofBen @DrEilidhMaria@CareQualityComm Unfortunately, event medicine / event first aid services are not CQC regulated activities (only ambulance services are if provided), so raising it with them may not be useful.
@drjgutt@be_nMD If you are posting about this case in detail so close to the time (presumably within 48-72 hours if there has not been time for neuro-prognostication), it is surely identifiable to family if they found your post?
I hope we see a robust response from @HNEHealth, as many would imagine that this message would be indicative of a deeper culture that devalues frontline medical staff. @ASMOFnsw
The whole point of @gmcuk is to keep patients safe from harm.
But what if, like OFWAT & OFCOM, it’s turning into another politically-neutered, failing regulator?
I cannot stand silently by as @gmcuk fails patients in the PA debacle.
Here’s why 👇
https://t.co/Zn8BkBstoG
Still in awe of the paramedics who somehow got an IV in me after I was down for >10 minutes due to cardiac arrest. It was 4am, dark, and their hazmat suit face shields were fogging up. Sounds impossible.
@MEHtheNurseTwin@pete_stubbs1@c3convertase I'm sorry, amazing nurses have caught errors I have made many times (including very silly errors on my part) - the core of this post is that doctors (particularly in the UK) are feeling a lack of respect, and you must see that a meme like that may not be as funny to us.
@MEHtheNurseTwin@pete_stubbs1@c3convertase That isn't even the quote from scrubs! Additionally, the change to the quote makes no sense, 10mg may be a reasonable dose for a patient when given slowly / incrementally and the blood pressure addressed simultaneously - hypotension is not a contra-indication for analgesia.
@thomaswoodcock Additionally, while some delegates are indeed from England (and organised leave well in advance of IA being announced), the conference is being held in Scotland, where no strikes are taking place, with many Scottish delegates unaffected by the current strikes.
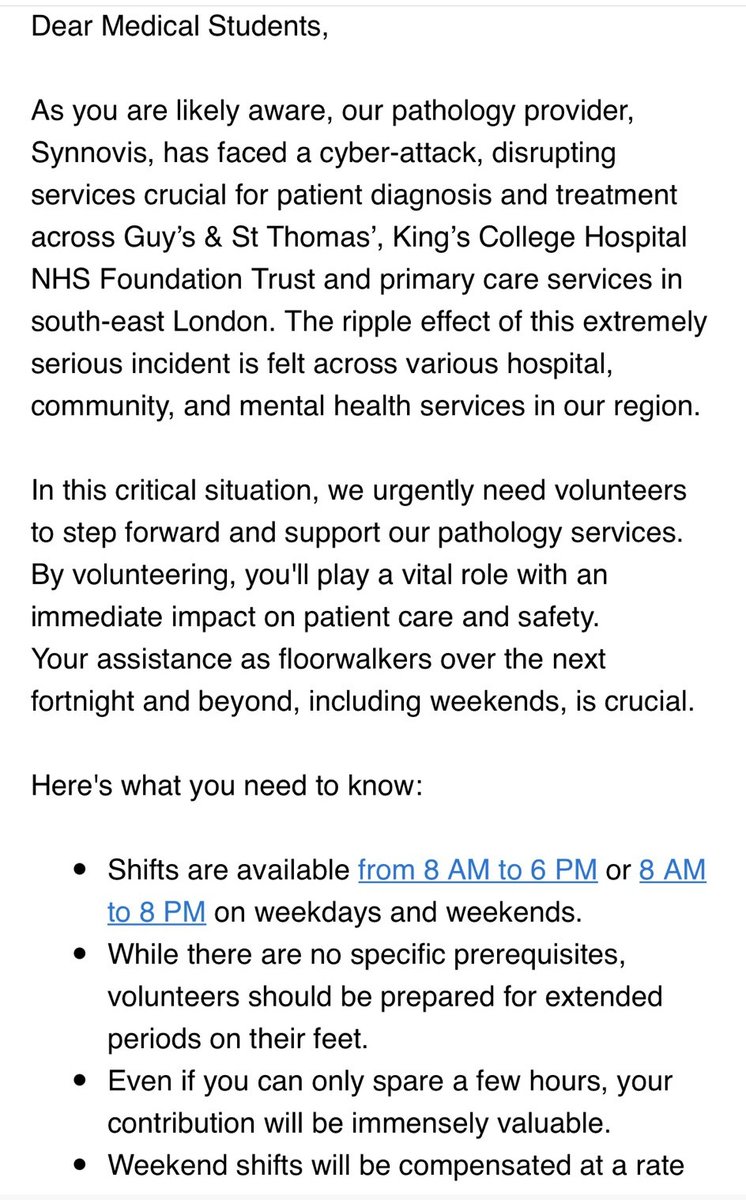
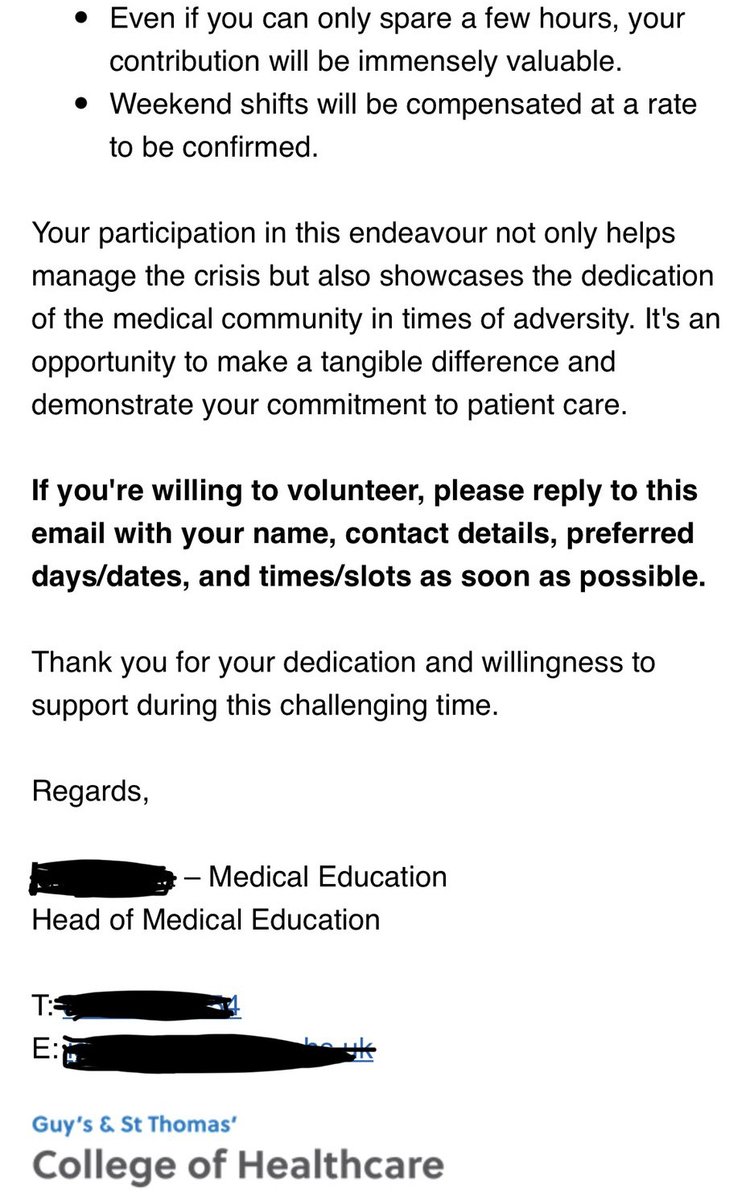
Asking medical students to volunteer doing things with little /no educational value to compensate for the failure of a service contracted to a private provider is unacceptable. They should be offered a wage for this work, and preferably the bill should be paid by @SYNLAB_UK
🚨 NEW: Medical students have been drafted onto wards in the wake of the NHS cyber attack. They will work as floor walkers, hand delivering blood tests to and from the crippled pathology labs. Bosses at @GSTTnhs say disruption will last "at least 2 weeks" 1/2
@EM_Dr_Jacklin In Aus, was used routinely by haem for bone marrow biopsy, although I have not seen it used in the UK for that indication (haem team seemed to want to use opioid +/- benzodiazapine for BMAT).
This video of an AA at a @gmcuk event about the loopholes in their scope of practice, apparently allowing AAs to provide remote site anaesthesia (IR) with distant supervision and up to 4:1 supervision, deserves more views. Obvious patient safety risk!
https://t.co/LkXeWqnRnL
@CLWillis0@JonBedford You are correct (bases like amines become protonated and ionised at pH below their pKa), Peck and Harris have made an error.
In case they read this - there is also an error in the structure of diamorphine on page 130 (putting methoxy groups instead of acetyl groups).
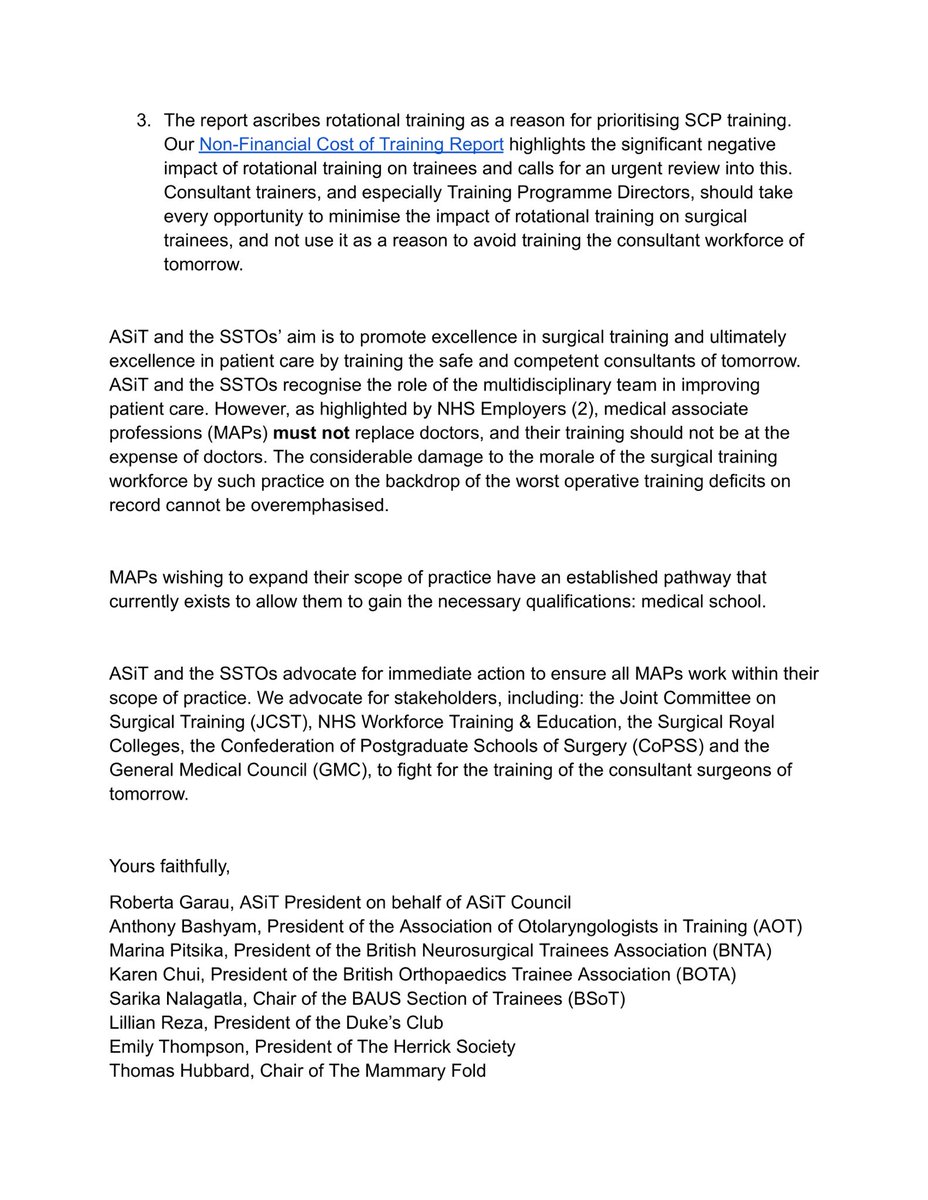
ASiT and the Surgical Specialty Training Organisations have released a joint statement in response to a recently published in The Annals of the Royal College of Surgeons England
What should be the #priorities in delivering surgical care?
Share with us your thoughts
🔗 https://t.co/ZmmfWbQy0s
2) This study is n=1, with no comparison data for their patient population. Despite this, the conclusion states that lap choles can be "performed safely and effectively with low complication rates" by SCPs.
Is this a valid conclusion, generalisable to all SCPs?
Probably not.
Lots of interest in this paper published in an RCS England journal looking at the safety of a (single) surgical care practitioner performing lap choles - a 2 thought thread 🧵 https://t.co/bv4JQQaskr
1) Is it acceptable that no ethics review was required for a study examining the safety of an intervention (in this case an alternative workforce providing surgery)?
Was this not a novel solution with an unclear safety profile?