Don’t chase aldosterone levels to decide who gets an MRA in HFpEF.
Check renin instead.
Renin <21 mU/L → high-sodium, hypertensive phenotype → may derive outsized benefit from combo MRA + SGLT2i therapy
Precision medicine in HF is getting real. 🎯
#MedTwitter#HeartFailure
🔍 Looking for a simple way to test for 🫁 recruitability during MV?
Bastia, @ERezoagli, & colleagues evaluate the value of a simple compliance ratio…
https://t.co/Rb5OQqpGUF
…you may be surprised! 😮😳
#journal_CHESTCritCare#OpenAccess
Unexplained dyspnea? Here’s the new ESC framework for diagnosing HFpEF — and it goes way beyond a basic echo 🧵
From Landsteiner et al., Eur Heart J 2026, a stepwise domain-based approach
4/
The mystery becomes how thrombosis formation in mechanical valves differs from that of atrial fibrillation or venous thromboembolism (VTE).
💡Because, as it turns out, the mechanism of thrombosis is NOT exactly the same in all situations.
https://t.co/7fP0XUyCFM
🫀 What happens when long-term low-dose #digoxin is suddenly withdrawn?
Blinded withdrawal analysis from the #DECISION trial presented at #HeartFailure26 by Prof. Peter van der Meer:
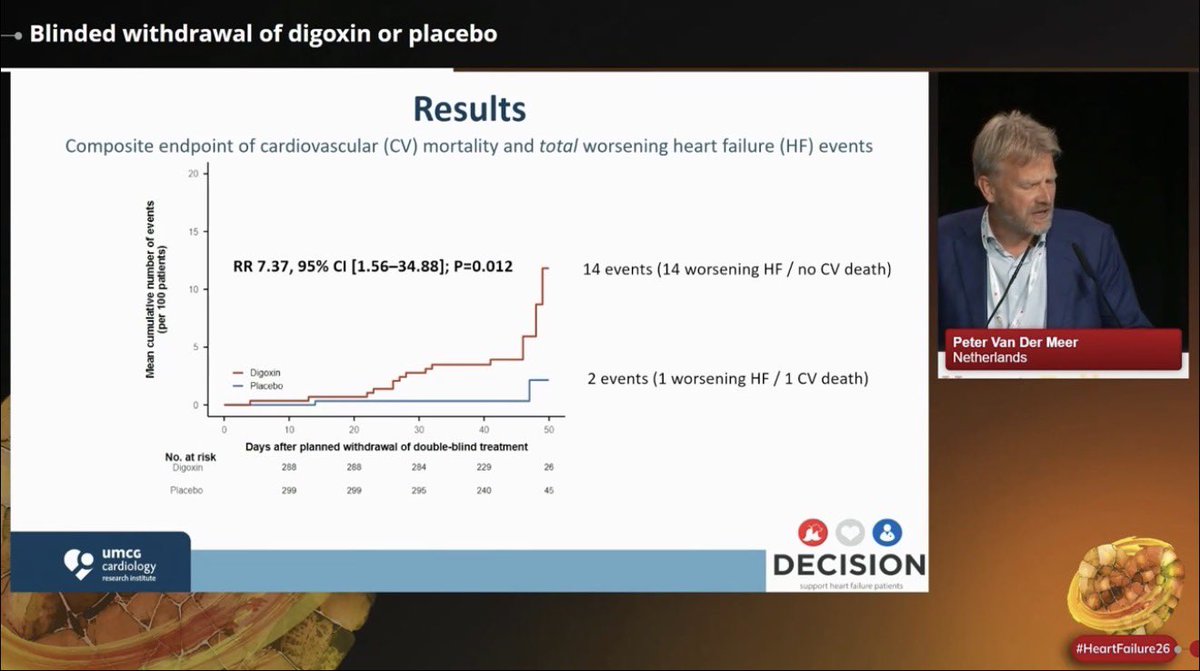
📍Digoxin withdrawal was associated with a ~7x increase in worsening HF events over just 6 weeks
📍14 worsening HF events occurred after digoxin withdrawal vs only 2 events in placebo withdrawal
📍Withdrawal was accompanied by: ⬆️HR,⬇️ SBP, ⬆️NT-proBNP, ⬇️eGFR
📍⚠️caution when stopping long-term low-dose digoxin in pts with HF & LVEF <=50%
@escardio@HFA_President@jozinetm
🧠🌡️ Temperature control in acute brain injury is evolving and the paradigm shift is important
For years, neurocritical care focused heavily on therapeutic hypothermia.
Cool the brain. Reduce metabolism. Improve outcomes.
The physiology made perfect sense.
But modern evidence is forcing the field toward a far more nuanced and physiology based approach.
📉 One of the most important concepts from this review
Fever itself may be one of the most underestimated secondary brain injuries.
Not simply a symptom.
A pathophysiological amplifier.
Across:
• Traumatic brain injury
• Ischemic stroke
• Intracerebral hemorrhage
• Subarachnoid hemorrhage
• Post cardiac arrest encephalopathy
Hyperthermia consistently correlates with:
❌ increased cerebral metabolic demand
❌ excitotoxicity
❌ oxidative stress
❌ cerebral edema
❌ intracranial hypertension
❌ worse neurological outcome
The review highlights that contemporary practice is moving away from indiscriminate hypothermia toward:
✅ controlled normothermia
✅ continuous temperature monitoring
✅ early fever detection
✅ minimization of temperature variability
⚠️ Important clinical nuance
Hypothermia still has physiological effects.
It can:
• reduce cerebral metabolic rate
• lower intracranial pressure
• attenuate excitotoxicity
But physiology alone does not guarantee improved outcomes.
This is one of the central lessons from:
• EUROTHERM3235
• TTM2
• EuroHYP
• INTREPID
The review elegantly demonstrates the recurring disconnect between: 🧪 physiological success
and
👤 patient centered outcome improvement
🫀 Perhaps the strongest practical message
Temperature management should not be viewed as: “A standalone neuroprotective therapy.”
It should be viewed as: “A modifiable physiological domain within brain centered intensive care.”
That distinction matters enormously.
Because it reframes temperature control as part of:
• multimodal neuromonitoring
• cerebral metabolism optimization
• ICP management
• seizure prevention
• oxygen delivery matching
rather than simply “cooling patients.”
📊 The figure on cerebral metabolism is excellent
The review illustrates how:
• fever
• seizures
• ischemia
increase CMRO₂ and worsen metabolic perfusion mismatch.
Meanwhile:
• sedation
• controlled temperature management
• selective hypothermia
can help restore coupling between cerebral oxygen delivery and metabolic demand.
🤖 Where the future may go
The next frontier is unlikely to be “cool everyone to 33°C.”
Instead:
• Multimodal monitoring
• individualized physiological phenotyping
• continuous metabolic assessment
• adaptive temperature targets
may finally identify WHICH patients actually benefit from deeper cooling.
Precision neurocritical care rather than protocolized hypothermia.
📖 Reference
Lavinio, A., Intensive Care Medicine. Advance online publication. https://t.co/AvJ7xIXikr
What treatments do we have in HFimpEF, HFremEF, and HFrecEF?
🔑 messages from #LynneStevenson at #HeartFailure26:
📍HFimpEF, remission (HFremEF), & recovery (HFrecEF) are distinct biological states with different relapse risks
📍HFimpEF is not the same as HFmrEF/mildly reduced EF
📍Treatment decisions should focus on the entire cardio-renal-metabolic journey, not EF alone
📍Phenotypes matter: HTN, diabetes, obesity, CKD & arrhythmias may still justify ongoing therapy
📍Genotype matters: for example #LMNA, #DSP, #FLNC, #RBM20 may influence relapse & arrhythmic risk even after EF recovery
@escardio@HFA_President@jozinetm@MarcoMetra@WilfriedMullens
The person who built Claude Code just showed exactly how to use it.
30 minutes. Free. Straight from Boris Cherny himself.
Bookmark this before you forget. Most people using Claude daily are missing 40+ features hiding in plain sight.
This single session is worth more than any $1000 course.
🫀📈 One of the most controversial debates in critical care may be shifting again.
This new 2026 systematic review and meta analysis in Annals of Intensive Care challenges that narrative directly.
The study analyzed:
📊 34 studies
📊 636,441 shock patients
📊 PAC, PiCCO and advanced hemodynamic monitoring guided resuscitation strategies
Main finding: ✅ significant reduction in in hospital mortality with advanced hemodynamic monitoring guided management (OR 0.66)
The strongest signal appeared in:
⚠️ cardiogenic shock particularly with pulmonary artery catheter guided therapy.
One of the most interesting physiological observations:
Patients monitored with advanced hemodynamic systems received:
• more vasopressors
• more inotropes
• more mechanical circulatory support
• more RRT
Yet mortality was LOWER.
That is extremely important.
This suggests the benefit may not come from the device itself, but from:
🧠 earlier recognition of instability
🧠 physiology informed escalation
🧠 more precise therapeutic targeting
In other words: better decision making.
The paper strongly supports a concept many intensivists intuitively recognize at bedside:
Not all shock is “vasoplegia plus fluids.”
Different hemodynamic phenotypes require:
• different vasoactive strategies
• different fluid approaches
• different escalation timing
• different mechanical support thresholds
Advanced monitoring may allow clinicians to move away from: “one size fits all resuscitation.”
Another important nuance:
The mortality benefit was strongest in cardiogenic shock.
The evidence in septic shock remains less definitive, although trends still favored advanced monitoring.
This may reflect an important reality: cardiogenic shock is fundamentally a hemodynamic disease.
One particularly valuable message from this paper:
The authors emphasize that modern AHDM is not simply “placing a Swan Ganz catheter.”
It is:
📌 integrating dynamic physiology
📌 interpreting perfusion targets
📌 understanding ventricular interactions
📌 identifying fluid responsiveness limitations
📌 tailoring escalation
Technology without physiology remains insufficient.
Interesting practical point:
The analysis did NOT show major increases in serious complications related to advanced monitoring devices.
That matters because procedural fear has been one of the strongest arguments against invasive monitoring.
My personal takeaway:
Critical care may be entering a new era where: precision hemodynamics returns to the center of shock resuscitation.
Not because catheters are fashionable again because modern shock management increasingly requires individualized physiology rather than protocolized averages.
📖 Reference
Nagy, L., Tóth, P. R., Turan, C., et al. (2026). Annals of Intensive Care, 16, 100071. https://t.co/z6ITSu4ubU
🫀 Why ventriculo arterial coupling may become one of the most important bedside hemodynamic concepts in critical care
For decades, ICU hemodynamic management has largely focused on isolated variables:
• MAP
• Cardiac output
• Ejection fraction
• SVR
• Lactate
But critically ill patients do not fail because of one variable alone.
They fail because the interaction between the ventricle and the arterial system becomes uncoupled.
⚙️ Ventriculo arterial coupling (VAC)
VAC integrates:
• Ventricular contractility → End systolic elastance (Ees)
• Arterial load → Arterial elastance (Ea)
The ratio Ea/Ees provides a physiological framework to understand cardiovascular efficiency and forward flow.
This is particularly relevant in:
• Septic shock
• Cardiogenic shock
• Mixed vasoplegic states
• Acute heart failure
• Dynamic ICU hemodynamics
📉 One of the most clinically important concepts
Blood pressure may remain preserved despite severe circulatory inefficiency.
A patient can have: ✅ “acceptable” MAP
❌ impaired stroke volume
❌ poor energetic efficiency
❌ inadequate tissue perfusion
Why?
Because excessive arterial load (Ea) relative to ventricular contractility (Ees) may maintain pressure while worsening forward flow.
This explains why pressure based resuscitation alone can sometimes fail.
🧠 The paper beautifully reframes septic shock physiology
Not all septic shock is the same:
🔹 Low Ea + preserved Ees
→ vasoplegic hyperdynamic sepsis
→ vasopressors appropriate
🔹 Low Ea + low Ees
→ septic cardiomyopathy with vasoplegia
→ vasopressor alone may worsen perfusion
→ requires combined vasopressor + inotrope strategy
🔹 High Ea + low Ees
→ afterload dominant cardiogenic physiology
→ excessive vasopressor escalation becomes harmful
📈 Perhaps the most exciting aspect
The authors demonstrate that VAC assessment is now feasible at the bedside using:
• Standard echocardiography
• LVOT VTI
• Simpson EF
• Blood pressure
• Doppler timing intervals
No invasive pressure volume loops required.
🤖 And the future?
AI assisted echocardiography + automated waveform analysis may allow:
• Continuous VAC monitoring
• Real time hemodynamic phenotyping
• Early uncoupling detection
• Precision vasoactive therapy
Potentially moving critical care from: “pressure normalization” toward “physiology targeted circulatory optimization.”
🎯 Clinical take home message
VAC does not replace: • MAP
• CO
• EF
It contextualizes them.
And that may be exactly what modern precision hemodynamics has been missing.
📖 Reference
Balan, C., Hearts, 7(1), 10. https://t.co/iJ2RboxAPe
Clinical implications 👇
• lowering HR may backfire
• vasodilation → ↓BP without ↑SV
• MRA & SGLT2i still beneficial
• (pacing only if CO-limited)
👉 Treat the pathophysiology, not the syndrome
I just read this outstanding review by Prof. Michael Pinsky:
👉 “The Effective Management of Shock: From Physiology to Guidelines to Personalized Medicine”
🧠 Key paradigm shift:
👉 Shock is not about numbers
👉 It is about tissue perfusion and cellular metabolism
⚠️ Three brutal truths (often ignored in daily practice):
1️⃣ Once organ injury occurs → we cannot reverse it
→ We can only limit further damage
2️⃣ Monitoring alone does not improve outcomes
→ Only actions linked to effective therapies matter
3️⃣ Guidelines ≠ patient care
→ The clinician’s physiologic reasoning remains central
📊 Why many “standard” approaches failed:
Targeting DO₂ “supranormal” levels → ↑ mortality
EGDT bundles → not superior to good early care
Fixed 30 mL/kg fluids → harmful in non-responders
👉 Lesson:
One-size-fits-all resuscitation is physiologically wrong
🫀 Modern hemodynamic thinking:
✔️ Fluid responsiveness matters (PPV, SVV, PLR)
✔️ MAP alone is not enough
✔️ Focus on:
Tissue perfusion pressure
Critical closing pressure (Pcc)
“Vascular waterfall” concept
👉 Increasing MAP ≠ improving microcirculation
🔥 Game-changing concept:
👉 Shock = failure of microcirculatory flow regulation
Even with:
Normal CO
Normal MAP
➡️ Tissue hypoxia may persist
🧬 The real goal of resuscitation:
❌ Normalize numbers
✅ Restore effective tissue perfusion early
✅ Avoid iatrogenic harm
💡 Where we are going:
Capillary refill time (CRT)-guided resuscitation
Personalized MAP targets
Dynamic physiology-based decisions
AI-driven precision resuscitation
📌 Take-home message:
👉 The future of shock management is NOT:
More fluids
More drugs
More devices
👉 It is: Better understanding of physiology + individualized care
🧠 And maybe the most important sentence in the paper:
👉 “The thoughtful bedside clinician remains the gold standard.”
#CriticalCare #Shock #Hemodynamics #ICU #Sepsis #PersonalizedMedicine #Resuscitation #Pinsky
I am an interventional cardiologist who treats heart disease for a living, including by putting stents.
This is my opinion on my tweet above. This is aimed at the general public. Long but worth the read:
First, some basics: Atherosclerosis (plaque formation) is a NATURAL PROCESS of life that begins in childhood. It progresses or can accelerate as you get older - as you live more life, due to genetics, and as you accumulate medical conditions such as high blood pressure, diabetes, live the "American" diet and lifestyle, etc.
Just like the plumbing in your home - a brand new house has clean, new pipes. Over 30, 40, 50 years of use, the pipes accumulate junk on the inside and can get clogged over time.
EVERYONE has some degree of plaque, some more than others. You cannot STOP the process. The goal of prevention is to find stuff BEFORE it causes problems, and to initiate measures to SLOW progression of plaque and to STABILIZE what you already have so it doesn't cause problems, i.e. a heart attack. The goal is to control it, live a long, good life, and die WITH heart disease and not BECAUSE of it.
1. CAC is a great SCREENING, preventive tool in APPROPRIATE patients to get a sense of how much coronary artery plaque one might have, to then better assess their RISK of future adverse outcomes like a heart attack.
The result of this test is NOT USED IN ISOLATION, rather it is used with OTHER tests, clinical history, etc to determine the best strategy to LOWER risk.
But in reality, a lot of people do not really *understand* RISK. They use this test, or are told by others to, as a way to "predict" *if* they will have a heart attack. I have lost count of the number of people who tell me "I have a CAC of 0 that means I won't have a heart attack, right?"
or
"I have a CAC of 1000! I was told I'm at imminent risk of a heart attack and I'm freaking out".
NO.
There is NO test in the world, and no human being that can tell you, if you are going to have a heart attack tomorrow, next week, next month, etc. Anyone who says they can is lying to you. You can't tell the future. If you want an ETA on if/when, ask God because only God knows.
But we CAN do is estimate RISK. A low CAC or CAC of 0 is great, and low risk, but not ZERO risk. A high CAC is indicates higher risk but does not mean 100% probability. Some people with low/Zero CAC have heart attacks and some people with CACs of 1000s never have a heart attack.
2. CAC measures CALCIFIED plaque - the advanced stage of plaque formation by which time plaque tends to become calcified and hard. It does NOT measure soft plaque - young plaque that has not had time to calcify yet. Therefore, while a CAC of 0 is reassuring, it DOES NOT MEAN YOU DON'T HAVE HEART DISEASE OR PLAQUE.
Generally, soft plaque can be "unstable" or "vulnerable" plaque which is often responsible for heart attacks, instead of the more stable, calcified type.
Carnivore bros in their early 30s and LDLs of 180 will often flaunt their CAC of 0 and say look! I’m good!
No. Doing a CAC on an average, healthy 30 year old with no family history is silly because the CAC will LIKELY BE ZERO. THEY HAVE NOT HAD ENOUGH TIME FOR PLAQUE TO CALCIFY YET. In fact, they can be layering soft plaque because of their LDL of 200 and have no clue. It can give people a false sense of security. I have put stents in enough 40 year olds with heart attacks with a 0 CAC score in the past to know this. It would also be silly to think that if you have a CAC of 0 you can continue to smoke and you're good - I don't think anyone thinks that.
Which is why when I have 30 year olds in my clinic with uncontrolled lipids, hypertension etc, I don’t do a CAC score. It will likely be 0. But i’m not going to just let them accumulate plaque until they get a CAC years later and finally they have a positive test and then we talk about risk factor control. That’s silly. I aggressively control all these risk factors EARLY in life.
3. The calcification *itself* does not necessarily cause a heart attack or stroke - like I mentioned earlier, these are typically very stable, hard plaques and less likely to cause a heart attack than unstable, vulnerable soft plaque.
A CAC is still very useful because it helps you assess overall plaque *burden* and therefore, risk. Compared to someone with a lower CAC score, someone with a higher CAC may have an overall higher BURDEN of atherosclerosis (including both calcified and non calcified). And a higher burden of plaque indicates higher risk.
3. CAC is not always = blocked artery.
A common misconception is that if you have a high CAC score that automatically means you have significant percentage blockage (50, 60, 70+ %) in your arteries. No. CAC should be seen as a marker of atherosclerosis and not blockage. A CAC test *cannot* tell you if you have a 70% blockage. You need a coronary CT or a coronary angiogram for that. Plaque can accumulate in many ways, and the arteries of the heart often adapt (“remodeling”) to accommodate that plaque WITHOUT causing a significant obstruction of the actual lumen of the artery, so blood flow is still relatively unimpacted. Obviously this is only to a limit, and eventually the plaque starts to protrude into the lumen and causes a significant blockage.
Don’t get me wrong, obviously a high score increases the chances of a significant blockage but this is not gospel. There are people with scores in the 1000s and all their plaque is in the wall of the artery, and the artery itself is wide open - there is no need for a stent or bypass for that. Conversely, people with low scores can have a significant blockage in an artery. Life is unpredictable and bizarre shit happens all the time.
4. A higher CAC does not automatically = further testing or a stent
This is another big misconception that people struggle with. For a lot of people who get this test - the average, *asymptomatic* person with a higher CAC score, the answer is to STOP further testing, and just manage risk factors aggressively. That’s it.
People say "but doc what if I have a heart attack? Why don't we look for an actual BLOCKAGE?"
You don’t typically need a stress test if you are asymptomatic. You don’t need a coronary angiogram or CCTA to look to see if there is a percentage blockage. Why? Because whatever plaque you do have has been ACCUMULATED OVER YOUR LIFETIME and is STABLE. You had it 2 months ago, even 6 months ago.
If you are ASYMPTOMATIC, it is just sitting there, NOT CAUSING PROBLEMS (yet). We found it, great, now we do things to reduce the risk that it causes problems 10, 20, 30 years down the line. Again, no one can predict if/when a heart attack happens. You could have had a heart attack months ago, when you had all this plaque but didn't even know about it.
Like I said earlier, atherosclerosis is a NATURAL process of life and EVERYONE has some degree of plaque. There are many people in your life, just walking around with severe plaque but they have no idea because it hasn’t caused problems for them, YET. They are at risk, of course.
If I did a coronary angiogram procedure for everyone (with or without a positive CAC), I would find some degree of blockage in most people. Even a significant blockage! But if this is STABLE and CHRONIC, generally there is no need to put a stent to open it up.
Because in stable heart disease, the heart often adapts in many ways. Stents generally do NOT help you live longer, they do not reduce the chance of a heart attack in the future. They really only just make people FEEL better, IF they have symptoms and IF their symptoms are caused by the blockage. If you’re asymptomatic, a stent is likely not going to do anything for you and you’re probably just incurring the risk of an invasive procedure without any significant meaningful benefit.
Opening up a stable blockage won't necessarily stop a heart attack in the future because you may have some soft, vulnerable unstable plaque somewhere else in the arteries that is not causing a significant % blockage in the artery, but decides to act up one day and cause a heart attack.
Obviously a heart attack is an acute condition with sudden 100% closure, and stents help save lives, and your heart muscle. But many people with heart attacks ALSO have chronic (even significant %) blockages in other arteries that were just bystanders. These blockages didn't cause problems and were found incidentally. They were present months, years ago, and the person probably didn't even know
Consider this analogy: the drain under your kitchen sink. When it clogs, it doesn't happen overnight. It happens over weeks and months. There may be a 50% clog but the drain works fine. But then as the clog progresses, the flow slows down over time and finally stops. That is STABLE. A heart attack is like someone throwing something in to your toilet and now you have a clogged toilet and an emergency.
Obviously, there are caveats to this - some people with high CAC need further testing, and may even need bypass surgery, depending on how high the score is, their risk factors, their history, and the type/severity of blockages. But *generally* speaking, this is not true for the AVERAGE person. I have done no further testing for people with high calcium scores, and conversely the full shebang for people with low scores. It depends.
All this sounds great in theory, but in practice, reality is very different. Influencers peddling CAC scores have meant that people are now getting these who may not be appropriate for them, and then they are getting a lot of downstream testing and unnecessary procedures (ie stent) that they DO NOT NEED.
People also, understandably, have anxiety. It can be hard to accept that they have a high calcium score and I do not recommend any further testing.
This is all understandable of course. No one wants to have a heart attack. I obviously think everyone should educate themselves and their loved ones about heart disease and take an active role to prevent disease, but we have to recognize there can be significant harm with indiscriminate, inappropriate use.
Bottom line: Prevention is KEY, and we need to do a LOT MORE of it. CAC scores are great tools, but need to be used and interpreted appropriately.
Disclaimer: Very simplified explanation, written quickly, educational only, and not medical advice. Discuss your specific case with your doctor. your doctor may disagree with me, and that's fine too! Do what is best for you! Thanks for reading!
The Role of Chloride in Cardiorenal Syndrome: A Practical Review
CCR Journal Watch - tracking the critical care literature daily
https://t.co/Sp06oA6IDG
Emerging Therapies: Levosimendan
🧪 Calcium sensitizer + vasodilator
🫁 Improves hemodynamics in PH-HFpEF
📚 Studied in small trials (HELP trial)
Still investigational — may be considered in advanced PH phenotype
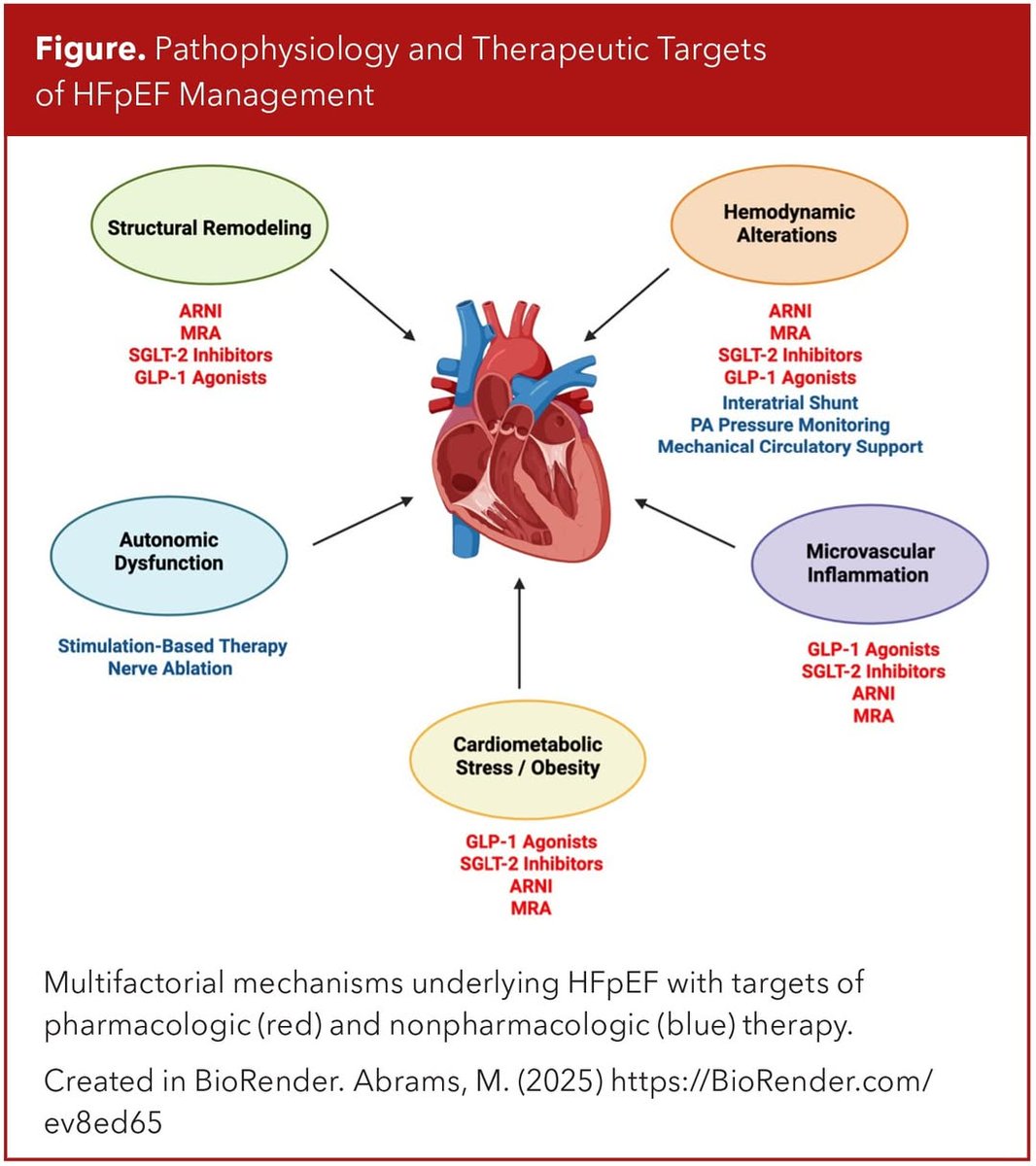
HFpEF ≠ “nothing to do” — we have therapies
There’s no Class I therapy for HFpEF yet. But we do have options that work — and are guideline-endorsed.
2022 AHA/ACC/HFSA HF Guidelines:
•SGLT2 inhibitors = Class 2a
•ARNi / ARB / ACEi = Class 2b
•MRAs = Class 2b
Key mimics to rule out before labeling HFpEF
🚩Constrictive pericarditis
🚩Infiltrative cardiomyopathies (amyloid, Fabry)
🚩Pulmonary HTN
🚩Valvular disease
🚩Volume overload from CKD
🧠 Think critically — not all dyspnea + EF 55% = HFpEF