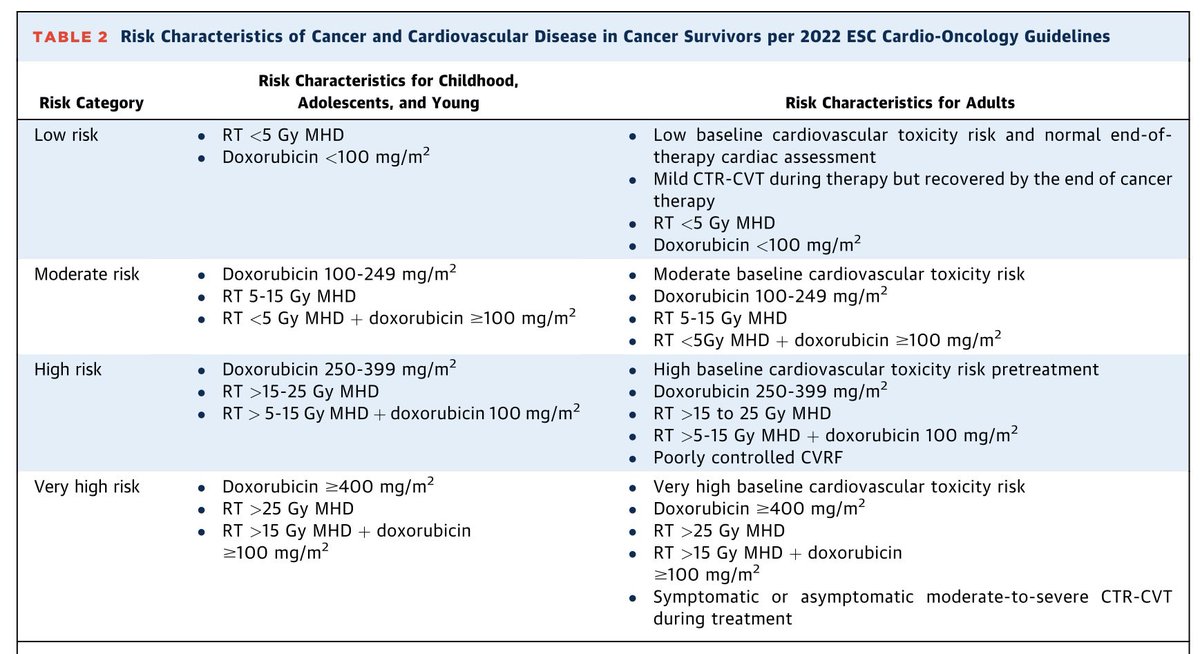
🧵 ¿Te bloqueas al interpretar un ECG con marcapasos? 🫀
No eres el único.
Si no estás habituado, distinguir un funcionamiento normal de una disfunción puede ser complicado.
Hay una regla sencilla que puede ayudarte en segundos: el algoritmo TBC 👇
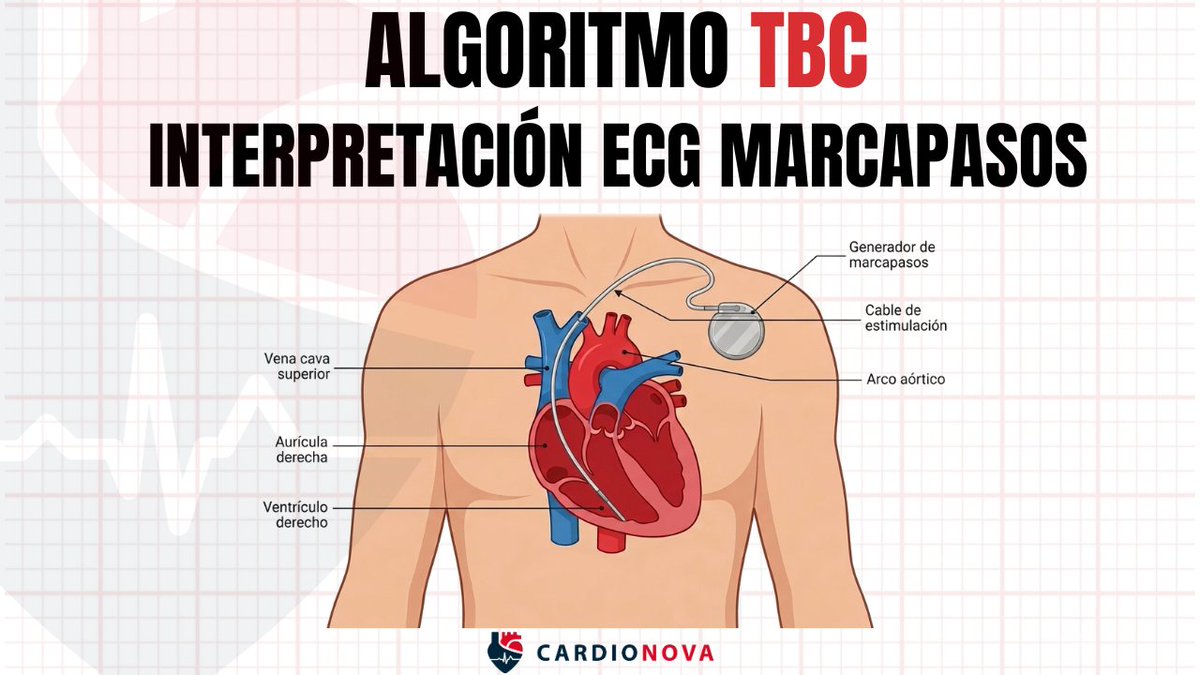
Published today, the first-ever clinical practice guideline on cardiovascular-kidney-metabolic syndrome from the American Heart Association and @ACCinTouch.
Cardiovascular-kidney-metabolic (CKM) syndrome staging is recommended for youths and adults to prevent CKM syndrome stage progression, to tailor therapy to absolute risk, to reduce cardiovascular events and loss of kidney function across the life course, and to promote CKM syndrome stage regression through lifestyle changes and weight loss.
The diagnosis of CKM syndrome stage requires assessment of metabolic health, kidney function, and cardiovascular risk factors, which enhances the identification of frequently unrecognized or asymptomatic CKM conditions.
✍🏼 @ChiadiNdumele@HeartDocSadiya@kardiologykazi@noshreza@virani_md@biykemb@NutritionHF@mandeepbajaj65@KatherineTuttl8@RangaswJ@lisaVWMD@KBreathettMD@EmoryFamMed@ShoaClarke@mad_sters@jmortonmd@sripalbangalore@AnumSaeedMD
In today's @TheLancet there are 3 papers on cardiometabolic disease: biology, epidemiology, prevention/treatment.
The sobering and all to common story from womb to tomb conveyed in this graphic
https://t.co/rVs2Yz97NC
https://t.co/OpuJTia0bC
https://t.co/i714onXoCG
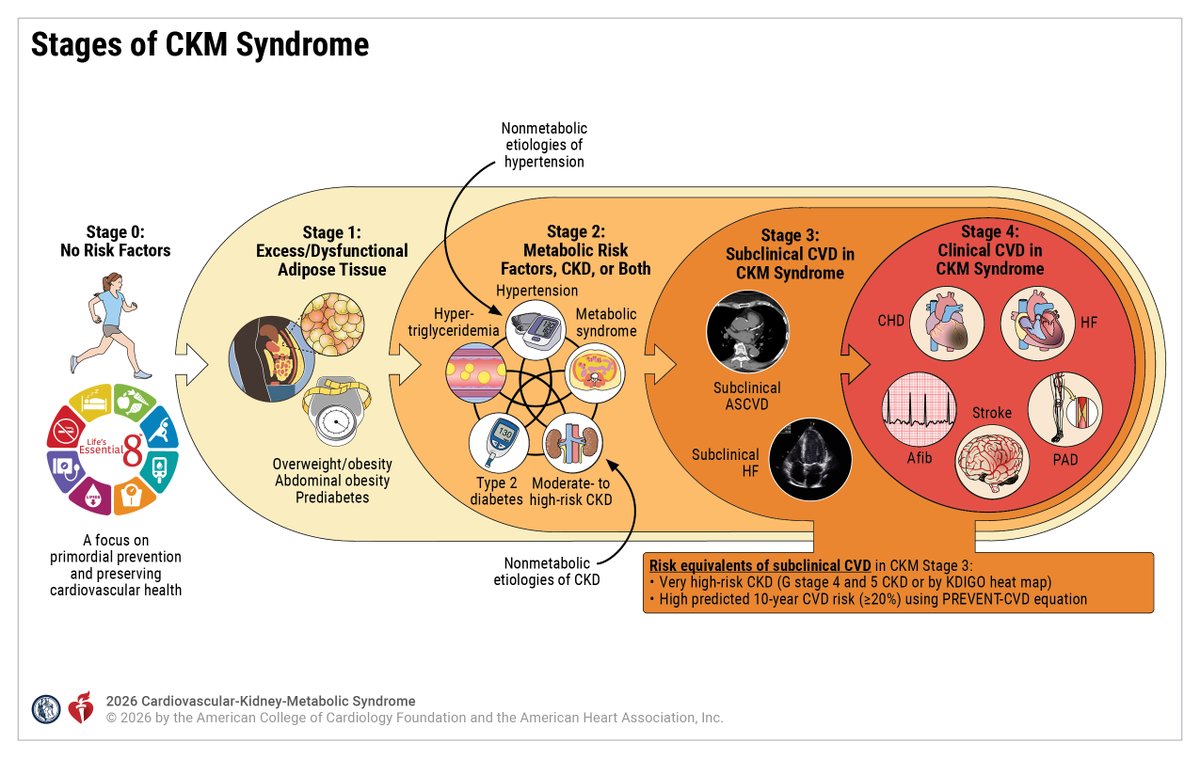
Cardiovascular considerations AFTER cancer therapy🫀
The final paper in a 3 part #JACCCardioOnc Expert Panel series exploring cardiovascular care before, during, & after cancer therapy
Cancer survivors remain at risk for future cardiovascular events throughout their lifespan.
Key contributors include:
🫀Pre-existing CV risk factors: Lifestyle, genetics, family history, race/ethnicity
🫀Cancer treatment-related factors:
📍Cardiotoxic therapies
📍Pharmacokinetic factors
📍Epigenetic changes
🫀Emerging CV risk factors
📍Insulin resistance
📍Dyslipidemia
📍Hypertension
📍Reduced exercise capacity
🫀Long-term survivorship requires a multidisciplinary approach involving oncologists, cardiologists, cancer rehabilitation, primary care physicians, & geriatrics.
Read more in @JACCJournals :
https://t.co/UZjR180Quh
#CardioOncology
Identification and management of non-obstructive high-risk coronary artery plaque
Please read the article and enjoy an in-depth interview between @jhfrudd and the first author, University of Edinburgh's Dr Craig Balmforth
Publication - https://t.co/j3ZQk2CNPa
Podcast - https://t.co/qPPLSvTdhj
Venous vascular pharmacology: how does it contribute to #HFpEF?
This review discusses current literature on the vasoactive effects of #EDRF and #EDCF in the venous vs. arterial systems, in both preclinical and clinical models on #HFpEF
https://t.co/2jjJkp38qn @ESC_Journals
Use of Predicted Risk and Expected Benefit to Guide Decision-Making in #CKD Syndrome for the Primary Prevention of CVD: A Scientific Statement From the @AHAScience and @ACCinTouch
https://t.co/ooxNw3WCmi
@CircAHA
📌2026 AHA/ACC/ADA/ASN Guideline for the Prevention, Detection, Evaluation & Management of Cardiovascular-Kidney-Metabolic Syndrome
#CaReME#CRM#Guidelines#PositionPaper
🏋️♂️ ¿Cuánto entrenamiento de fuerza necesitas para vivir más?
📊 Estudio con 147.374 personas seguidas durante hasta 30 años:
⏱️ 90-120 min/semana de fuerza
✅ ↓13% mortalidad total
✅ ↓19% mortalidad cardiovascular
✅ ↓27% mortalidad por enfermedades neurológicas
Y aquí viene lo interesante:
⚠️ Más NO fue mejor.
Superar los 120 min/semana de entrenamiento de fuerza no aportó beneficios adicionales sobre la supervivencia.
Terapia antitrombótica después de la cirugía de revascularización coronaria (CABG). 💊💥🫀
💊Aspirina: la piedra angular. La aspirina reduce la oclusión de injertos y los eventos CV sin incrementar significativamente el sangrado postoperatorio.
✅Mantener aspirina perioperatorio.
✅Reiniciarla dentro de las primeras 24 horas tras cirugía (idealmente antes de las 6 horas).
✅Continuar de forma indefinida a dosis bajas (75-100 mg/día).
💊💊¿TAP Dual? En pacientes con alto riesgo isquémico y bajo riesgo hemorrágico, puede considerarse aspirina + ticagrelor o clopidogrel durante 12 meses (indicación mas fuerte en SICA que en SCC) para mejorar la permeabilidad de los puentes venosos (reducen MACE pero aumentan 🩸).
✅Reiniciar TAPD tan pronto como el riesgo de sangrado esté controlado.
✅Mantenerla durante 12 meses.
✅Ticagrelor o prasugrel son preferibles a clopidogrel por su mayor reducción de eventos isquémicos y mortalidad.
📄🆓️⤵️ @ESC_Journals 💯
https://t.co/IcdxvQsTD9
https://t.co/SeTF6YUsXm
Cardiovascular considerations DURING cancer therapy🫀
The second of a 3 part #JACCCardioOnc Expert Panel series exploring cardiovascular care before, during, & after cancer therapy.
Recommendations for #CardioOncology care during cancer treatment:
Cardioprotection🛡️:
📍ACEI/ARB, beta-blockers, & statins may be considered to prevent ⬇️LVEF with anthracyclines 📍Consider dexrazoxane or liposomal doxorubicin for high cumulative anthracycline dose or LVEF <50% 📍Implement strategies to minimize cardiac radiation exposure
Surveillance🖥️:
📍Echo for anthracyclines & HER2-targeted therapies 📍Troponin & ECG for patients receiving ICIs
📍Prompt treatment & evaluation for high suspicion of ICI myocarditis 📍Blood pressure monitoring for VEGFi, BTKi, & ALKi therapies 📍Lipid monitoring for lorlatinib
Permissive cardiotoxicity⚖️:
📍Continue HER2-targeted therapy in selected patients with mild LV dysfunction, but need to evaluate risk & benefits 📍ACEi may be reasonable in patients with ⬆️ troponin during anthracycline therapy 📍Nitrates and/or calcium channel blockers can be considered to treat & rechallenge selected patients with 5-FU/capecitabine vasospasm, with close monitoring
Read more in @JACCJournals:
https://t.co/gxcpXpcDP2
Cardiovascular considerations BEFORE cancer therapy🫀
The first of a 3 part #JACCCardioOnc Expert Panel series exploring CV care before, during, & after cancer therapy.
🫀Goals of CV evaluation Prior to cancer therapy:
📍Identify and treat subclinical CVD and cardiovascular risk factors 📍Optimize management of pre-existing CVD and cardiovascular risk factors 📍Perform targeted risk assessment to help inform cancer treatment decisions 📍Establish baseline cardiovascular function 📍Optimize primary prevention therapies 📍Plan cardiovascular surveillance during treatment
🫀Current tools include clinical assessment, biomarkers, 12-lead ECG, #EchoFirst, & risk scores
🫀Important evidence gaps includes cardiotoxicity mechanisms, impact of pre-treatment CV evaluations on clinical outcomes, validation&implementation of risk scores, & the role of AI.
Read more in @jaccjournals: https://t.co/cTCY0Acg99
#CardioOncology
🚨 Nuevos grados de severidad en el corazón derecho según la ASE.
Cambia la evaluación del VD, la AD y la arteria pulmonar:
❌ menos “normal/anormal”
✅ más grados de severidad
✅ más valor pronóstico
Si quieres estar al día en Eco, este hilo es para ti 👇🏼 🧵#CardioNova#Eco