It’s why I say that 2019 me is dead. I have the same hobbies and the same family, but I’m not that person anymore. That person was optimistic and believed in the inherent goodness of humanity, from which a small percentage of people deviated.
The pandemic taught me the opposite is true, that people are only as good as the amount of inconvenience they can withstand.
It doesn’t change how I interact with others, but has seismically shifted how invested I become. It is what it is.
A friend passed this to me, saying it might be helpful - it's about getting help on Long Covid from your GP, it's for a UK setting, but some of it will be applicable anywhere - read the note at the end for more too.
"I work in AI. I used it to research and write my mum a letter about her Long COVID. Her GP called her the next day after 3 years of being dismissed!
*Reposting here as myself since it blew up in another support group and people really want help with this… feel free to add/DM me.*
So I work in AI, specifically in healthcare tech. So when my mum had been fobbed off by her GP for the third year in a row about her Long COVID, I figured I should actually do something useful with what I know.
This isn't about gaming the system or bending rules. Everything I'm sharing here is publicly available on NHS and government websites. I just used AI to find it, understand it, and turn it into something a GP couldn't easily brush off.
Here's what most people don't know. The NHS publishes detailed guidelines that GPs are expected to follow. NICE published a specific Long COVID guideline called NG188 that sets out exactly what a GP has to do when a patient comes to them with ongoing post-Covid symptoms. Most patients have never heard of it. Most GPs don't follow it unless someone pushes them on it.
The other thing most people don't know: verbal dismissal is easy to ignore. A formal written letter that references specific guidelines creates a paper trail. The GP now has a documented duty of care they're expected to respond to. It genuinely changes everything.
My mum is 61. Not remotely tech savvy. She would never have found any of this herself. I spent about 20 minutes using AI to pull the relevant guidelines, match them to her situation, and draft a letter. She sent it to her GP by email on a Tuesday. Her GP called her on Wednesday afternoon. First time in three years a GP had called her. She now has a referral to a Long Covid clinic and a written management plan, after years of being told it was probably anxiety or just her age.
Posting her letter below with her details redacted. Copy it, adapt it to your situation, send it by email not in person. You need a timestamp. You need a record. That's what actually forces a response.
───
[Her letter, personal details redacted]
████████████████
████████████████
████████, ██████
██ ██████ 2025
Dr ████████████
████████████ Surgery
████████████████
████████, ██████
Re: Formal written request for Long COVID assessment and personalised management plan
Dear Dr ████████,
I am writing to formally request appropriate assessment and management for post-COVID-19 syndrome (Long COVID), and to create a written record of this request for my medical file.
I contracted COVID-19 in ████████ 2022 and have experienced the following ongoing symptoms for over three years:
• Severe fatigue and post-exertional malaise, symptoms worsen significantly following any physical or cognitive exertion
• Cognitive dysfunction, difficulty with memory, concentration, and word retrieval
• Breathlessness disproportionate to exertion
• Heart palpitations and episodes of tachycardia
• Disrupted sleep despite significant fatigue
• Generalised pain and joint discomfort
These symptoms have substantially impaired my ability to work, maintain daily activities, and quality of life.
CLINICAL BASIS FOR THIS REQUEST
NICE guideline NG188, COVID-19 rapid guideline: managing the long-term effects of COVID-19, was developed jointly by NICE, SIGN and the Royal College of General Practitioners. It applies to any patient with new or ongoing symptoms four or more weeks after acute COVID-19.
Under NG188 section 5.2.1, GPs are expected to use a multidisciplinary approach to guide rehabilitation, including physical, psychological and psychiatric aspects of management.
Under NG188 section 5.2.2, GPs must work with the patient to develop a personalised rehabilitation and management plan, which must be recorded in writing. NICE states explicitly that healthcare professionals are expected to take this guideline fully into account. This is not optional guidance.
Under GMC Good Medical Practice (2024), where a GP cannot adequately manage a patient's condition, they are required to refer to a specialist with the relevant expertise.
Under the NHS Constitution, I have the right to be referred to an appropriate specialist where my GP is unable to provide the required clinical management.
I have not received a personalised management plan or specialist referral in three years of presenting with these symptoms.
WHAT I AM FORMALLY REQUESTING
1. A holistic clinical assessment consistent with NICE NG188, including physical, psychological and functional domains
2. A personalised rehabilitation and management plan recorded in writing, as required under NICE NG188 section 5.2.2
3. Referral to the Long COVID clinic or appropriate multidisciplinary rehabilitation service
4. A written response to this letter within 14 days
I would like this letter to be added to my medical record. I am not requesting anything outside published NHS guidelines. I am asking for what those guidelines state I am entitled to receive.
Yours sincerely,
████████████████
Date of birth: ██/██/████
NHS number: ███ ███ ████
Based on: NICE NG188 (January 2024) | GMC Good Medical Practice (2024) | NHS Constitution (2023)
*Verify current guidelines at https://t.co/1G9ny67PrQ before sending.*
───
Same approach works for basically any condition where you're being dismissed. MCAS (I am currently writing myself a letter to escalate my own issues with this), fibromyalgia, EDS, POTS, chronic fatigue. The escalation pathways exist for all of them, most people just don't know how to use them.
If it’s useful I could build a tool that does this automatically for you. You answer a few questions about your condition, it finds the relevant guidelines and drafts the letter for you. If that sounds useful, DM me or comment. Happy to write one manually for anyone in the meantime.
Not medical advice! Keep seeing your GP. Call 111 if anything gets worse."
We didn’t defeat COVID-19—we redefined it.
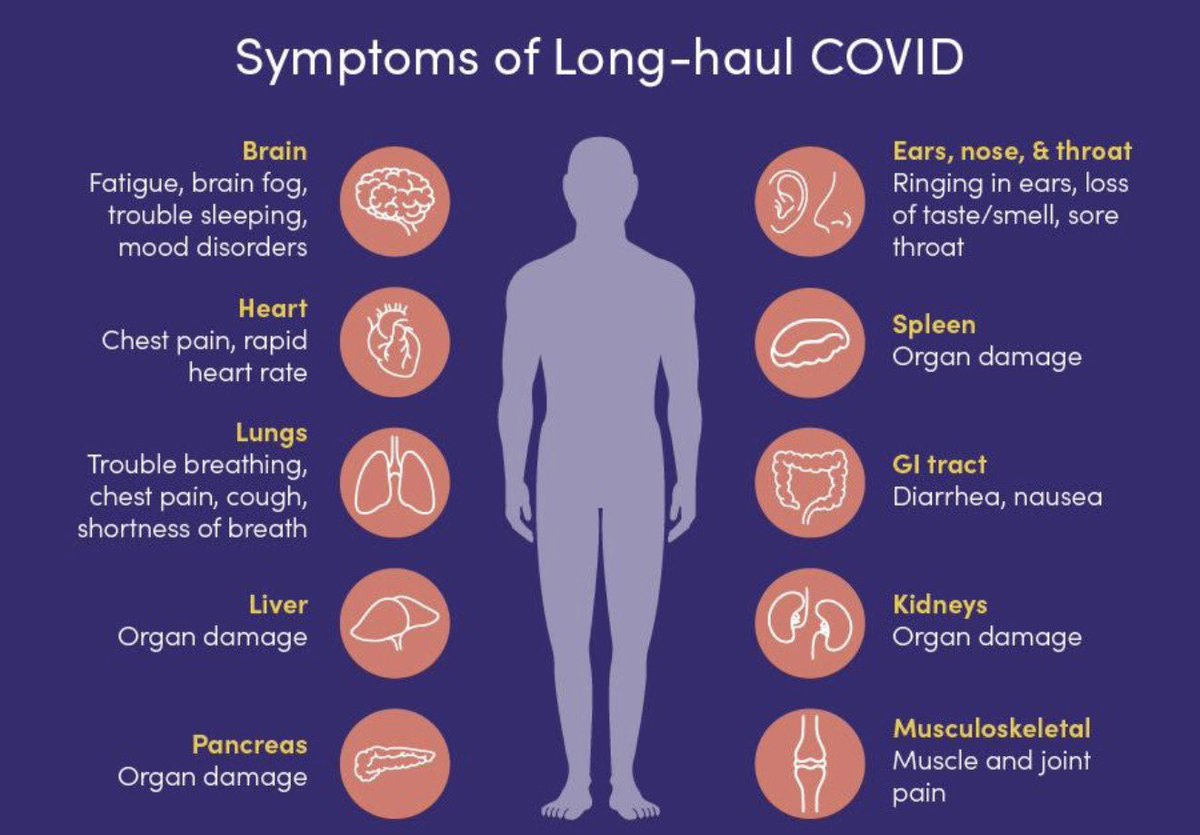
➡️ #LongCOVID now represents a mass disabling event, with lasting neurological, cardiac, and systemic effects that health systems are still failing to confront.
➡️ The pandemic didn’t end—it shifted into LongCOVID, a chronic, disabling condition affecting millions.
➡️ From lungs to brain, LongCOVID leaves a trail of persistent, multisystem damage long after infection.
➡️ What was once an acute crisis is now a silent, long-term epidemic hidden in everyday clinics.
➡️ A new report estimates that medical costs for the treatment of longCOVID patients will average US$11-billion annually across the 38 countries
➡️ Ignoring LongCOVID means overlooking the true, ongoing burden of COVID-19.
https://t.co/mwQh7sZxA5
COVlD: Week of Apr 20, 2026 (PMC, US)
Levels are at their lowest in nearly 3 years, but unfortunately with a high baseline of >200,000 estimated new daily infections.
Very High = WV (1 site only)
Moderate = MS (limited data) & Guam
All others low/very low
🧵THREAD 1/7
Researchers warn of severe long-term damage to the brain after Covid following new study
« people who developed long-term neurological symptoms after Covid also showed increased levels of phosphorylated tau, a protein linked to early brain degeneration » https://t.co/H0uciGaWbq
After the participants left the launch workout, my coworker announced to the room:
“Yeah, I really think I had Covid 2 weeks ago. My poor son coughed for so long afterward. I lost my voice. There was no way I could teach like that.”
Then the tone shifted, and I could feel the dark, deceptive energy moving in. As the conversation slithered into shadows, a coworker slipped in seamlessly,
“Yeah I now have to take allergy medicine every day. It’s good to switch them up every day and keep them on rotation.”
Relief washed over their faces. They had chosen a safer fear. A smaller monster. One they could name without consequence.
Another voice joined almost eagerly, “Yeah I actually take Benadryl in the mornings now. Doesn’t even make me sleepy.”
Relief continued to spread, reassured and collective.
The original coworker slipped in, voice suddenly sharpened.
“Oh no!! Not that Benadryl. I remember reading articles saying it’s causing early onset dementia!!”
I felt it boiling inside me. Something dark and intelligent was threading through the conversation, nudging it off course from what we had all just heard. The denial, the coordinated pivot, and the unspoken agreement to bury it.
And then,
the words escaped from me like a scream into the void.
“NO IT IS NOT BENADRYL CAUSING EARLY ONSET DEMENTIA. IT IS COVID!!”
Everything stopped, as if time was frozen. Jaws dropped in slow motion. Eyes widened into black, glassy voids. Every head turned toward me at once, bodies locked in perfect unison. For one frozen second the room became a hive mind staring back, rabid and starving, ready to tear the truth apart with teeth and silence.
And layered into that split second, something else briefly showed through.
A quiet, collective terror.
Not of the illness itself, but of dragging it fully into the light where it could no longer be softened into something smaller, safer, or more manageable.
Because once spoken truthfully,
awareness spreads.
And that very awareness starts to crumble the fragile architectures people have built to keep functioning.
Their eyes stayed on me too long. Wide and unmoving. As if I had broken a rule no one admits exists.
Then, just as quickly, everyone sealed back over.
A laugh, and a shrug. Someone changed the subject.
The room collectively rebooted.
But I knew it was not relief.
It was suppression.
Because the truth is not misunderstood.
It is recognized and buried alive.
And Covid is not just a passing illness. It is the thing no one is allowed to call upon even as it reshapes everything we are and everything we will become.
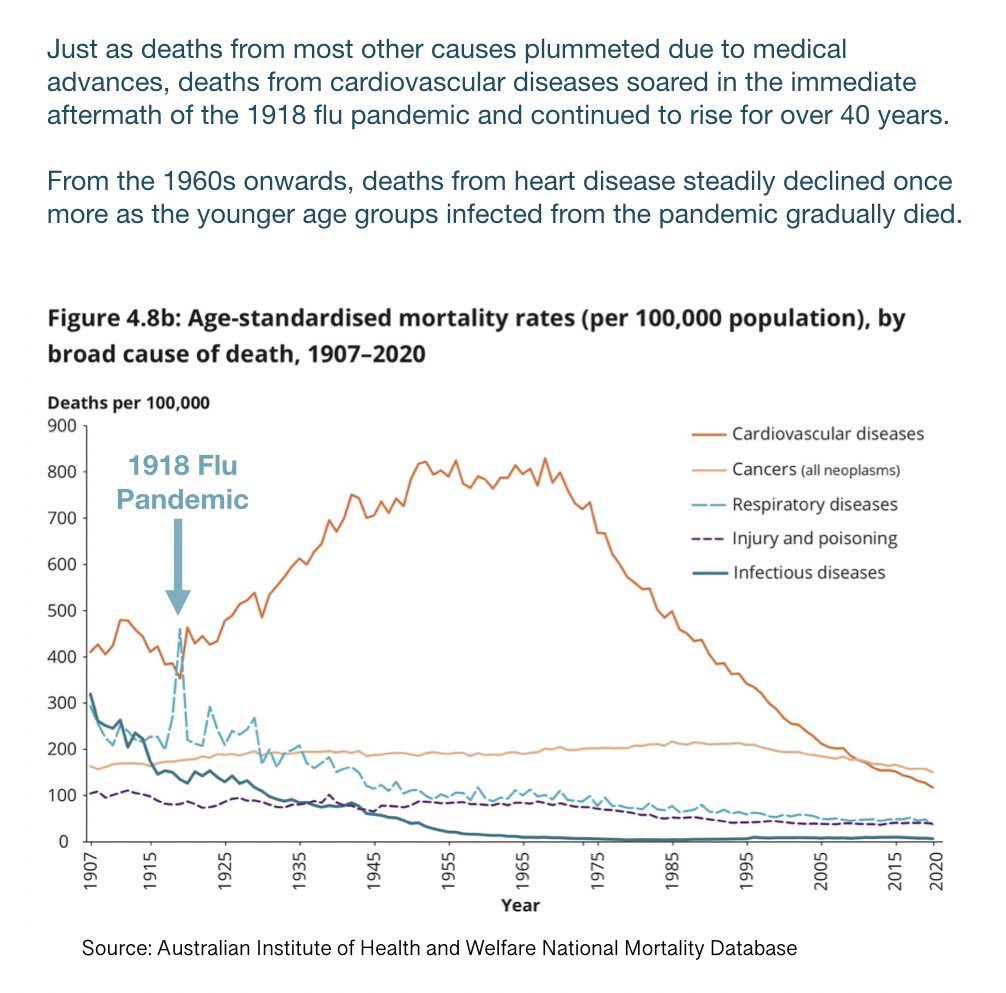
Did you know that, in the aftermath of the 1918 flu pandemic, deaths from cardiovascular diseases soared and continued to rise for over 40 years?
From 1960 onwards, deaths from heart disease steadily declined as the younger age groups infected during the pandemic gradually died.
Advocacy isn’t posting. It’s doing.
I’ve stayed quiet at times because I hate the spotlight. I don’t want to be here. I want to play tennis with my daughter. I want to take the mask off, take my wife on a date, and not think about any of this.
But I can’t unsee what I’ve seen. And I can’t unhear what I’ve heard.
I’ve spent over 1,000 hours listening to people with Long Covid. Every story. Every symptom. Every dismissal. Every collapse.
Everything.
And once you understand how this actually works, how it dismantles human functioning, and how individuals have dismantled awareness of this disease and its prevention, you don’t get to walk away.
Let’s get something straight about advocacy.
Advocacy is not clout chasing. It’s not selling protocols. It’s not cosplaying as a clinician. It’s not gatekeeping illness categories. It’s not belittling patients. It’s not blocking people who ask hard questions. And it’s definitely not showing up for a day or a month of awareness and disappearing the rest of the year.
Advocacy is doing.
What have I actually done?
I’ve written to professional organizations across behavioral medicine, cognitive science, and education pushing for masking, remote accommodations, and evidence-based guidance. I’ve drafted letters supporting disability claims grounded in scientific evidence. I’ve advocated for children and families facing harassment for masking.
I’ve spoken at school board meetings. I’ve created templates for families navigating unsafe environments. I’ve directly contacted educators, administrators, policymakers.
I built an Illinois Air Quality Dashboard linking indoor air quality, absenteeism, and public health risk. I’ve developed tools for people trying to stay safe in an environment that has abandoned prevention.
I submitted a PCORI grant to center patient voices in research design and to build infrastructure for trials. 50+ hours of work. No guarantee of funding. Still did it.
I don’t have Long Covid.
This work pulled me away from my primary research area. It complicates my career. It costs time, energy, and honestly, peace.
I haven’t earned a cent from Long Covid.
I’ve been asked to join podcasts. I declined. I’ve been asked to write for organizations. I declined. I’ve been asked to lead grant efforts for trials. I declined.
If I don’t clearly see how people with Long Covid benefit, I don’t invest my time. If I detect conflict of interest, I decline.
But I have stayed here because I know how to evaluate evidence. I know how to build systems. And I’ve listened long enough to know who is being failed.
There are people out there who are ignored, misdiagnosed, talked down to, sold false hope, or told this is all in their head.
That part, I won’t tolerate.
What’s broken right now?
We have grifters selling snake oil. Researchers collapsing distinct conditions into convenient narratives. Professionals minimizing or dismissing patients.
I’ve stepped back from certain spaces because many of them are no longer centered on patients.
At the same time, prevention has been erased. The disease itself is being erased. Both ends of an aerosol-transmitted disease. Same result.
And during moments where there should be unity, there’s fragmentation, ego, and noise.
The reality?
Entire countries are redefining conditions in ways that blur critical distinctions. People without medical training positioning themselves as authorities. Patients being told not to protect themselves.
And here in Illinois, we’re fighting just to get basic clean air education and AQ monitors into schools. A bill that might not even survive.
I’m not here to build a following. I’m not here to sell you something. I have donated to individuals and even helped raise over $1k for a charity (although, I'm not entirely sure to what extent that really helps families with LC).
I’m here because prevention matters. And patients deserve better. And the truth still matters, even when it’s inconvenient.
I’m continuing this work through infrastructure, tools, advocacy, and direct support. And I’ll be putting more of my own money into it.
I’m building something called LANTERN. More on that soon.
If you call yourself an advocate, ask yourself this:
What have you actually done to make someone safer, heard, or better supported?
Not talked about. Not posted about.
Done.
This space doesn’t need more voices. It needs more people willing to do the work.
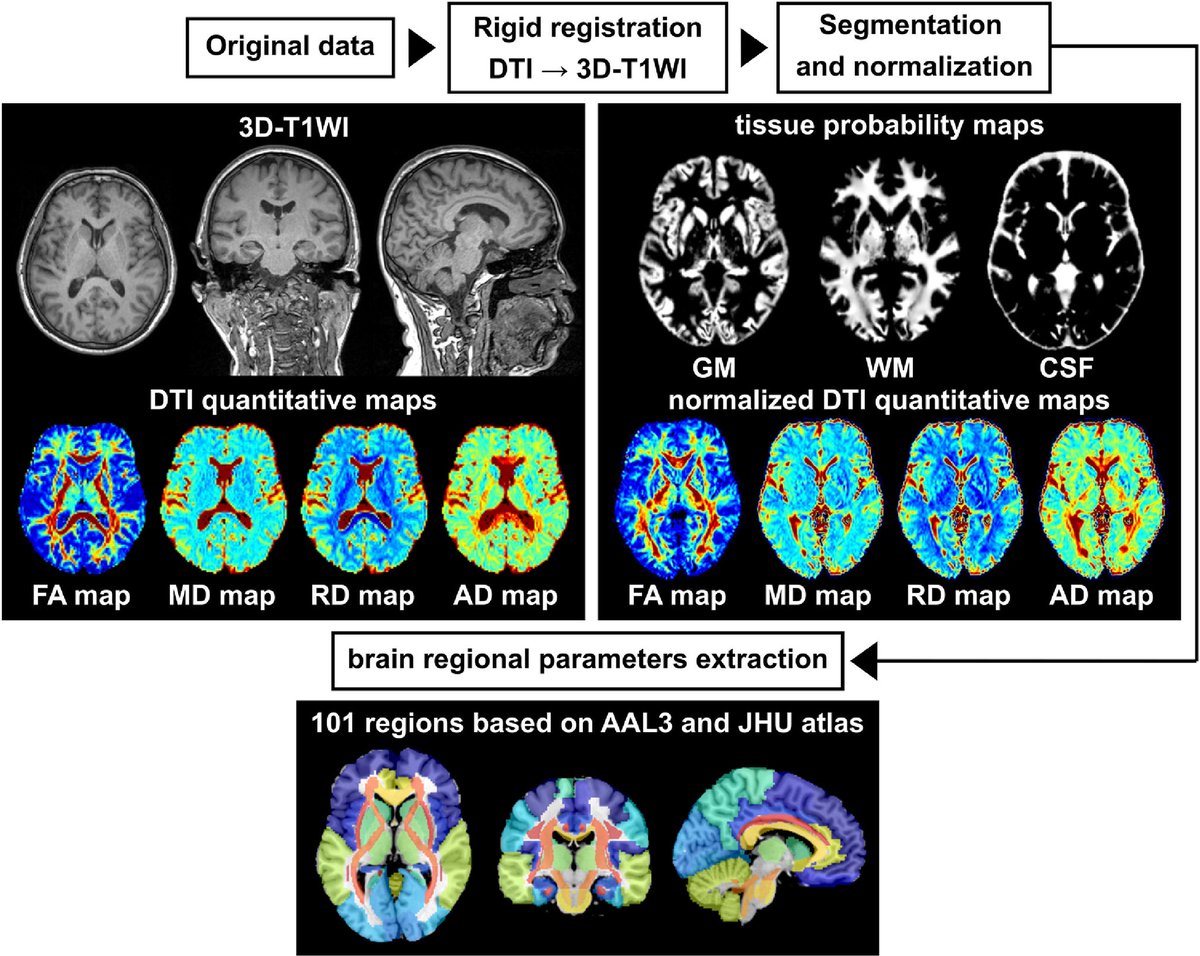
A review of 49 MRI studies shows that COVID-19 is associated with structural and functional brain changes.
➡️ Abnormalities are most commonly seen in the frontal, temporal, and parietal lobes, as well as the limbic system and subcortical regions.
➡️ These findings suggest widespread brain involvement, not limited to a single area.
➡️ The changes may explain both acute neurological symptoms and long-term effects (LongCOVID).
👉 COVID-19 is not just a respiratory disease—it has measurable, widespread effects on the brain
https://t.co/jh3xH1ZlIR
here's a good example of the "disjointing experience" in a tiktok video i just came across. this woman is doing rotations in a hospital & describes feeling a "post covid lobotomy" after every covid infection she has
Let’s be perfectly clear, the pregnant girls being held in the Texas ICE camp are children.
They’re not “young women”.
They’re kids.
If they’ve been impregnated after being locked up, every single ICE guard must be investigated for child rape.
The girls must be freed.
Teachers are often leaving the profession because they themselves have a hard time teaching. They have fatigue, brain damage, hard times paying attention and having patience with children, memory issues, processing speed issues, executive function issues from multiple Covid infections. How many infections have you had?
Giving adults and children unfettered access to Covid is the problem .
Classroom teacher here to remind everyone that this is cognitive decline caused by repeat COVID-19 infections.
Screen-less classrooms and conversations with parents have shown significant declines that can’t be explained with just the change towards screens
Early studies confirmed LongCovid patients have a lower quality of life than advanced cancer patients.
The CDC also confirmed this.
Then we deliberately normalized Covid & “accepted exposure,” because no one wants to pay for this.
A year ago, 48M Americans had LongCovid.
It’s not just one outbreak. Over the last few years, we’ve seen spikes in multiple communicable diseases; flu, RSV, TB, measles, strep infections etc alongside higher general sickness in the population
The magnitude and severity in groups that were previously low-risk is unusual
A group of my very dear friends came together to make this post, thank you to @alexandrite113 & Fran I’m not sure you’re on Twitter, and everyone who contributed. #longcovidawareness#longcovid
“You’re not just becoming disabled,” said Elle Seibert, 31, who has dealt with debilitating fatigue and cardiac symptoms since 2020. “You’re realizing how easily society at large and people in your life will abandon you when you cannot offer them things.” https://t.co/jVI9ruk1Re