The study, one of the first randomised-controlled trials to evaluate the use of AI-powered decision-support tools in trauma care, will see AI-TRiPS deployed across The London Trauma System, the largest integrated trauma network in the world which serves over 10 million people.
Working with colleagues across London and the UK, Queen Mary academics are launching a new trial looking at how AI can support emergency care outside of the hospital setting.
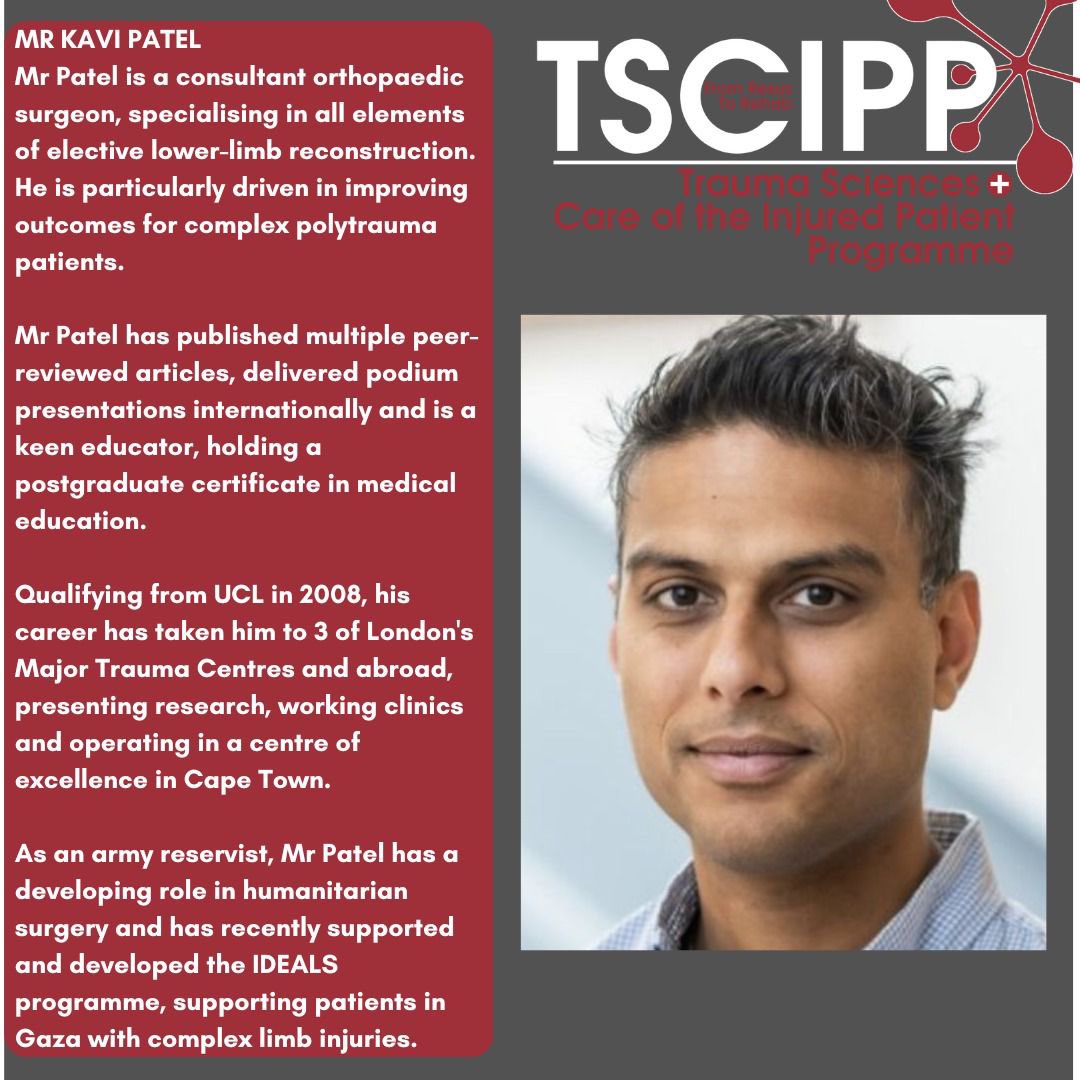
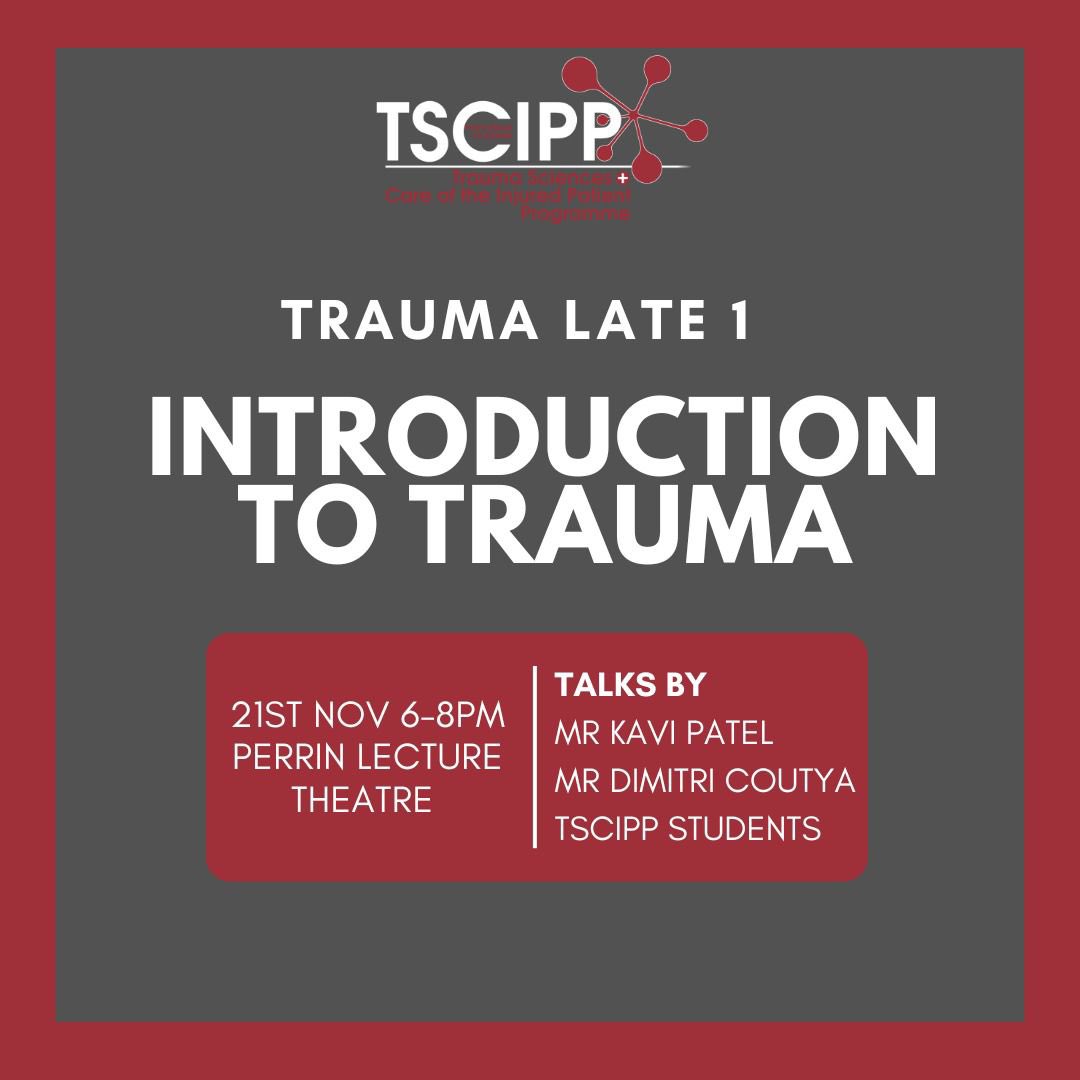
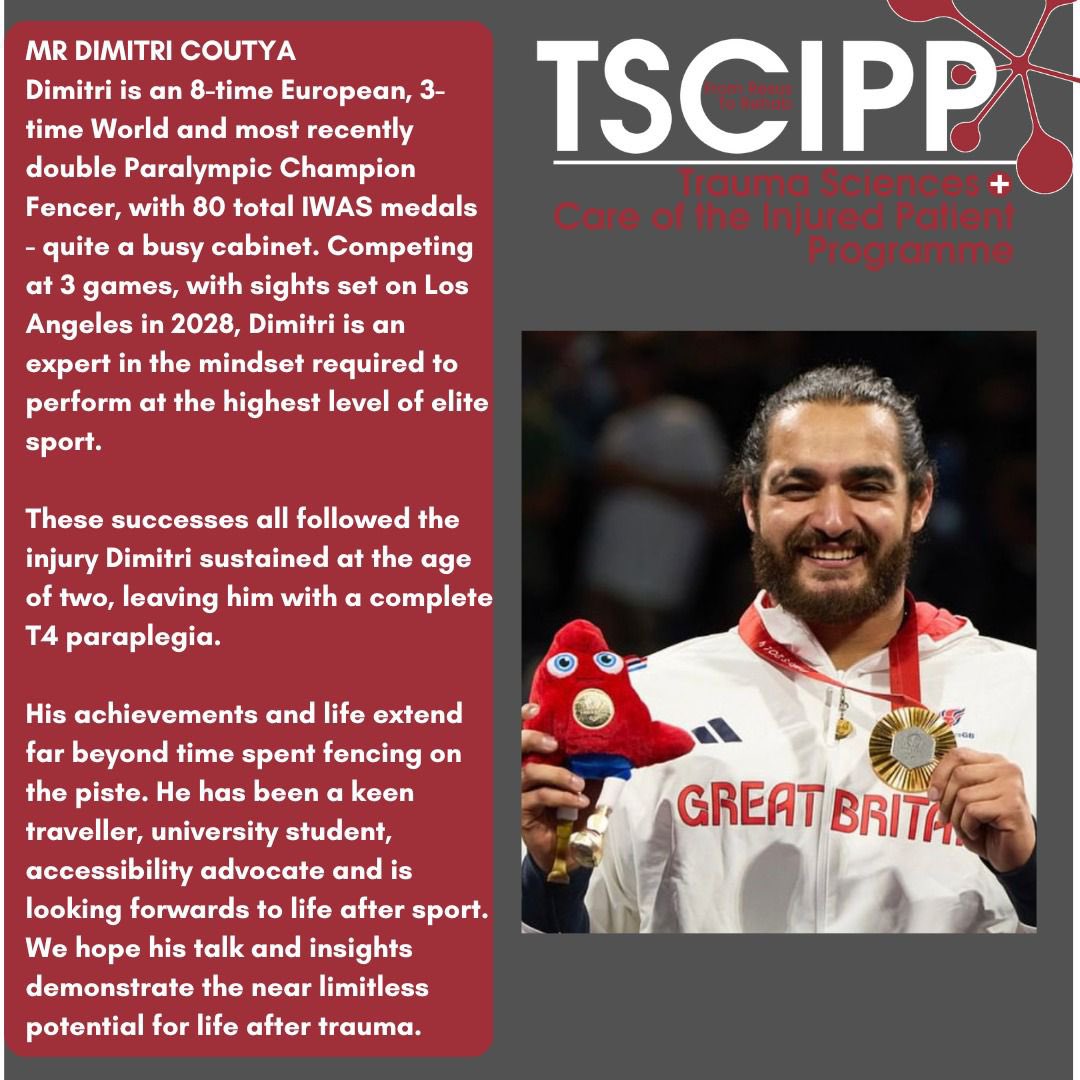
🚨 TRAUMA LATES ARE BACK! 🚨
Our first Trauma Late of the year as always is: ‘An Introduction to Trauma’.
Scroll through the post to have a look at our speakers for the evening. We hope to see you there! 🚁
Deaths from knife injuries would be more than double what they are now if it wasn't for advances in the science and practice of trauma care.
@BBCRadio4 describes how, in the course of 20 years, we've increased the number of people getting to hospital alive, and dramatically reduced the chances of death from major bleeding.
It's still 1 in 5 though.
Ooo thanks @aneelbhangu. You have great taste! :)
We put a lot of time and money into our website (and it never ends). But research without dissemination and impact may as well not have happened.
Also a momentous day for Andrea Rossetto @Andrea91Ross who successfully defended his PhD at the Centre for Trauma Sciences @QMUL. Kudos also to his supervisors @rossdavenport & Laura Green.
Andrea is our 23rd PhD @CommsC4TS. #strongwork
Clinical Trial Managers!
We have a vacancy within the Centre for Trauma Sciences at Queen Mary University of London for a Clinical Trial Manager to oversee our current studies (Phase 2a/b RCTs, Perpetual cohort studies and diagnostic test accuracy studies); and to help develop and institute future trials.
https://t.co/t5df4P35AS
This is a critical post for us and involves running very exciting but challenging trauma trials in both in-hospital and prehospital environments. We need someone with knowledge and experience of this space, who is enthusiastic and willing to engage with multiple teams locally, nationally and internationally.
Very happy to consider flexible working options and other adjustments. Due to the nature of the funding the post is advertised as being until March 2025, but we expect this funding to continue as it has done for several years previously.
OK that went well, I think 😎.
Here are my reading of the sessions:
SESSION 1: UK-REBOA
Most would say REBOA as currently delivered does not have a place in ED phase of care of major trauma patients thought to have non-compressible haemorrhage.
BUT:
? - Does it have a niche in the right patients - if only we could recognise them?
? - Would the results be the same for new techniques like partial REBOA
? - Has the right place always been prehospital / deployed situations? (given the caveats above)
We still don't have answers for non-compressible torso haemorrhage, and although there are other devices out there/on the horizon, they come with their own issues and are (far far) less rigorously evaluated.
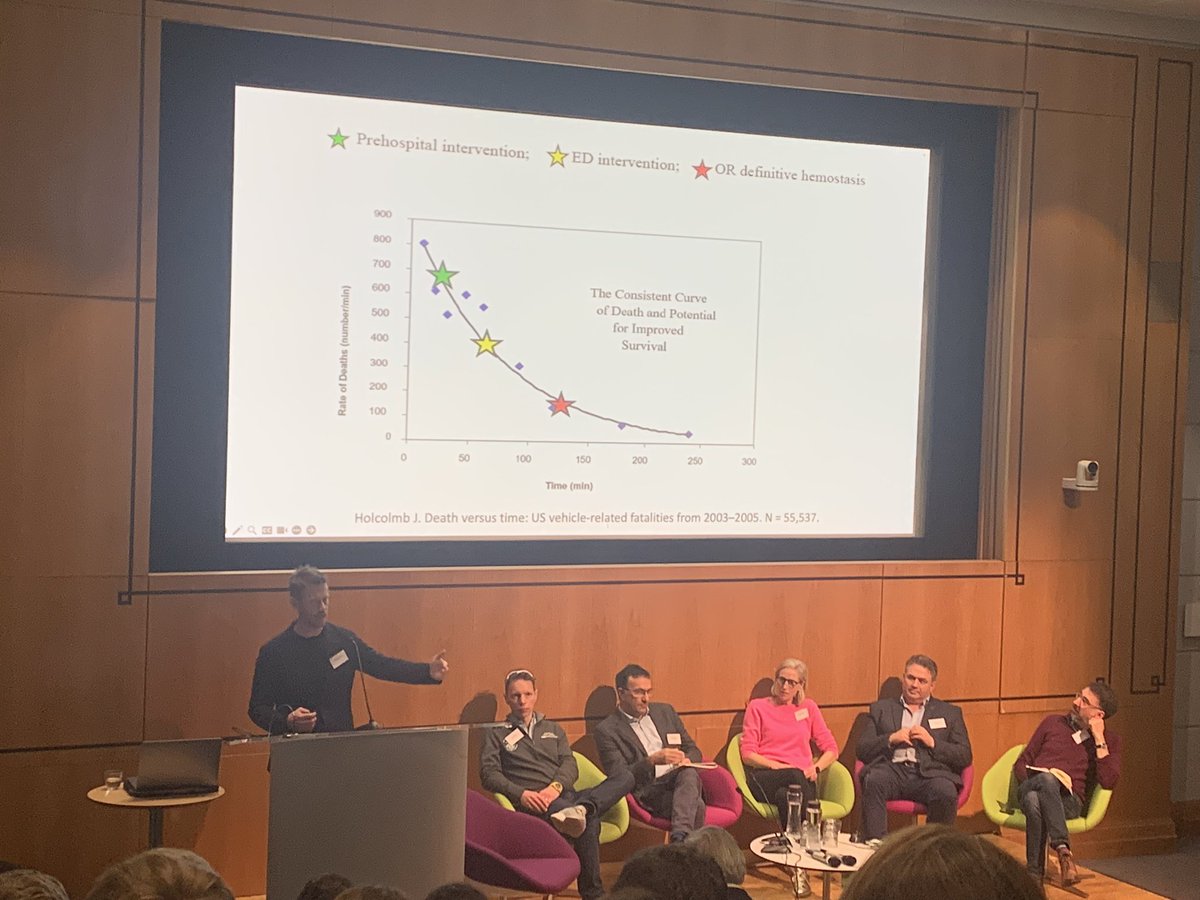
SESSION 2: THE BLEEDING PATIENT
TIME came up again and again.
Are we fast enough. Are we as fast as we think we are (no).
There are clear differences between different systems.
We need to consistently examine what we do and identify the opportunities to be faster.
If we had been faster - if we could be faster - would REBOA have worked?
Do we need a way to physically separate these patients from the wider ED/trauma population?
SESSION 3: CRYOSTAT2
There was general acceptance that high-dose cryoprecipitate (or fibrinogen concentrate) should not be given to all trauma patients on arrival.
Cryoprecipitate remains indicated when there is low fibrinogen, and is likely safe and effective when given empirically later in bleeding (eg after 8+ units RBCs).
Again patient selection is key. Point of care fibrinogen or equivalent ROTEM/TEG could guide treatment.
Probably a case now for all UK MTCs to have immediate point of care access to ROTEM & TEG.
Processes and human factors are as important if not more important than what we are giving.
Again hospital design and planning important.
We should examine/research moving away from blood-bank based therapies.
How do we audit and quality improve coagulation therapies. What should we be measuring to drive improvements?
DAY 2: DECISION MAKING IN TRAUMA
(I am going to do this day a disservice by summarising it so succinctly, but...)
Again and again on Day 1, the issues of patient selection came up, and the recognition that we don't have the tools to consistently do this, even in expert hands.
Decision making in trauma care is complex and nuanced and not easily explainable by the people who made those decisions. Uncertainty is higher at the times when the most critical decisions must be made.
There's a real opportunity for AI decision support. AIs (or SOFTWARE as we are encouraged to refer to these tools) cannot MAKE decisions. But they can potentially integrate multiple data points to "expose" the current state of the patient.
There are many many aspects to consider in moving from an in-solico prediction model to a real world widely used and trusted decision support tool, and no one has done this as yet, really, for anything in medicine.
The team @nigeltai and @ZBPerkins have put together at @QMULBartsTheLon are on their way to doing this.
PUBLIC ENGAGEMENT & INVOLVEMENT
There was a lot of enthusiasm for a programme of work to develop a "roadshow" of sorts that could be used locally in MTCs, TUs etc to showcase to the public how trauma care has improved over the last 15 years, especially through research-led changes an interventions. An opportunity as well to highlight local injury prevention activities, successes and innovations, and to highlight the important of things like bystander bleeding control training (first aid!). Check in with James @thepiercy if you have ideas / want to get involved.
THAT'S IT from the meeting - but the conversations will continue and we will explore how we can develop these into recommendations and policy (so good to hear everyone else's take-homes too). Thank you to everyone who attended and contributed, in person and online.🙏
Trauma Haemorrhage: What Now? @wellcometrust
Non-compressible haemorrhage @janjansenuk
Prehosp REBOA @robbielendrum
-time for a new RCT?
Military REBOA @nigeltai
-whole system implementation science key!
Time to haemorrhage control @paulvulliamy
-longer than you think!
1/2
Launching our Palliative and End of Life care guidance for older trauma patients today. Huge amount of work from the multi-specialty, inter-professional project team. Thank you! https://t.co/8EtBsn5k41
Immature platelets are highly active, but their role in outcomes after major trauma is unknown. Schofield, Rossetto et al found:
⏬immature #platelets early after injury🔼mortality
⏫immature platelets later timepoints ▶️organ failure/thrombosis @CommsC4TS https://t.co/lSLxup3XXI
Get a broad and critical understanding of the most up-to-date science and practice of #trauma care with our online #MSc in Trauma Sciences, delivered by experts from @CommsC4TS, @QMULBartsTheLon & the Royal London Hospital major trauma centre. Apply now: https://t.co/1R0QH1FyrX
A pleasure to host Fayez @EHAAT_ to undertake work towards his @CommsC4TS PhD in simulation related to major incidents @blizard_inst@QMUL Thanks to the team for taking part, and especially for the massive cake!! @BurrellLisa
Our @wellcometrust funded TOP-ART (Trauma Organ Protection - Artesunate) trial results just published in @yourICM.
Not the result we were expecting/hoping for but lots of learning for trauma and some potential flags for artesunate's use in malaria.
#strongwork@CommsC4TS and especially @JoMShepherd.
Thrilled to be at the launch of the NHS London Violence Reduction Academy, with Lead Martin Griffiths and @QMUL partners Martin Freestone, Heather McMullen and @karimbrohi. @QMUL_WIPH@blizard_inst