Haemodynamic equations are useful. But they also mislead.
Take:
CO = HR × SV
CO ≈ (MAP − RAP) / SVR
Both are mathematically true. But they can make the variables they contain look like the controllers of output.
Often they are not.
In the intact circulation, these equations describe the resolved state of the system. They do not, by themselves, tell you what is supplying energy, what is constraining flow, or what is actually limiting output.
That is one of the central themes of our review:
Energy, flow and pressure in the cardiovascular system: a narrative review of how the circulation works.
https://t.co/L19bsDCzr6
🫀📈 One of the most controversial debates in critical care may be shifting again.
This new 2026 systematic review and meta analysis in Annals of Intensive Care challenges that narrative directly.
The study analyzed:
📊 34 studies
📊 636,441 shock patients
📊 PAC, PiCCO and advanced hemodynamic monitoring guided resuscitation strategies
Main finding: ✅ significant reduction in in hospital mortality with advanced hemodynamic monitoring guided management (OR 0.66)
The strongest signal appeared in:
⚠️ cardiogenic shock particularly with pulmonary artery catheter guided therapy.
One of the most interesting physiological observations:
Patients monitored with advanced hemodynamic systems received:
• more vasopressors
• more inotropes
• more mechanical circulatory support
• more RRT
Yet mortality was LOWER.
That is extremely important.
This suggests the benefit may not come from the device itself, but from:
🧠 earlier recognition of instability
🧠 physiology informed escalation
🧠 more precise therapeutic targeting
In other words: better decision making.
The paper strongly supports a concept many intensivists intuitively recognize at bedside:
Not all shock is “vasoplegia plus fluids.”
Different hemodynamic phenotypes require:
• different vasoactive strategies
• different fluid approaches
• different escalation timing
• different mechanical support thresholds
Advanced monitoring may allow clinicians to move away from: “one size fits all resuscitation.”
Another important nuance:
The mortality benefit was strongest in cardiogenic shock.
The evidence in septic shock remains less definitive, although trends still favored advanced monitoring.
This may reflect an important reality: cardiogenic shock is fundamentally a hemodynamic disease.
One particularly valuable message from this paper:
The authors emphasize that modern AHDM is not simply “placing a Swan Ganz catheter.”
It is:
📌 integrating dynamic physiology
📌 interpreting perfusion targets
📌 understanding ventricular interactions
📌 identifying fluid responsiveness limitations
📌 tailoring escalation
Technology without physiology remains insufficient.
Interesting practical point:
The analysis did NOT show major increases in serious complications related to advanced monitoring devices.
That matters because procedural fear has been one of the strongest arguments against invasive monitoring.
My personal takeaway:
Critical care may be entering a new era where: precision hemodynamics returns to the center of shock resuscitation.
Not because catheters are fashionable again because modern shock management increasingly requires individualized physiology rather than protocolized averages.
📖 Reference
Nagy, L., Tóth, P. R., Turan, C., et al. (2026). Annals of Intensive Care, 16, 100071. https://t.co/z6ITSu4ubU
🍽️ ICU nutrition: we’ve been doing it wrong for years?
More calories
More protein
Earlier feeding
Sounds logical
But physiology disagrees
⚠️ The key update
High-quality RCTs now show:
❌ Early full-dose nutrition
→ NO benefit
→ Potential harm
Especially in:
• Shock
• Multiorgan failure
• High metabolic stress
👉 This is not neutral
👉 This is dangerous practice
🧠 Critical illness is not static
It evolves through metabolic phases:
1. Acute catabolic phase
2. Stabilization phase
3. Recovery phase
👉 Feeding must follow physiology
Not protocols
🔥 Phase 1: Acute catabolic
• High inflammation
• Insulin resistance
• Endogenous substrate mobilization
👉 The body is NOT ready for full nutrition
💡 Strategy:
✔️ Permissive underfeeding
✔️ Low protein
Why?
Because early overload leads to:
• Hyperglycemia
• Hepatic dysfunction
• Renal stress
• Impaired autophagy
👉 You are feeding dysfunction, not recovery
⚖️ Phase 2: Stabilization
• Inflammation decreasing
• Organ function improving
👉 Now metabolism starts to tolerate nutrition
💡 Strategy:
✔️ Slow escalation
✔️ Daily reassessment
⚠️ Red flags:
• Hypophosphatemia
• Hyperglycemia
→ Patient is NOT ready
💪 Phase 3: Recovery
• Anabolism returns
• Mobility improves
👉 NOW nutrition matters most
💡 Strategy:
✔️ Higher calories
✔️ Higher protein
✔️ Combine with rehab
👉 This is where you rebuild muscle and function
📊 The real takeaway
Nutrition is NOT:
❌ A fixed prescription
❌ A calorie target
It is:
✔️ A dynamic therapy
✔️ A metabolic intervention
🎯 The new principle
“Start low
Advance judiciously
Individualize throughout”
👉 Precision ICU nutrition
⚠️ Final thought
Overfeeding early harms
Underfeeding late harms
👉 Timing is everything
📚 Stoppe C et al. Curr Opin Clin Nutr Metab Care 2026
DOI: 10.1097/MCO.0000000000001186
In healthcare, the simplest actions save the most lives!
Congrats to our Theatre team for their outstanding Hand Hygiene Performance!
Their dedication to international safety standards helps prevent infections and keeps our patients safe.
#ActionsSaveLives#HandHygiene
🧬 Sepsis biomarkers: are we finally moving beyond CRP and PCT?
Sepsis is not just infection.
It is a dysregulated host response leading to multi-organ dysfunction.
And yet…
👉 Our diagnostic tools are still slow
👉 Our biomarkers are still imperfect
🧠 The current reality
We rely on:
• CRP → sensitive but non-specific
• PCT → better for bacterial infection, useful for antibiotic guidance
• Lactate → cornerstone for perfusion and prognosis
➡️ But none of them truly capture the complex biology of sepsis
📊 What is changing?
New biomarkers are emerging across multiple domains:
🔥 Inflammatory markers
• IL-6 → correlates with severity and mortality
• IL-10 → reflects immunosuppression
• TNF-α → early hyperinflammatory signal
⚙️ Immune cell markers
• CD64 → helps differentiate bacterial infection
• Presepsin → early diagnostic and prognostic potential
🧪 Metabolic markers
• Lactate kinetics still critical
• Metabolomics → early prediction of shock progression
🧬 The real revolution: multi-omics + AI
👉 Transcriptomics
👉 Proteomics
👉 Metabolomics
Combined with:
🤖 Machine learning
➡️ Allowing:
• Sepsis phenotyping (endotypes)
• Hyperinflammatory vs immunosuppressed states
• Personalized risk stratification
🚨 Critical insight
Sepsis is:
❌ Not one disease
❌ Not one pathway
❌ Not one biomarker
➡️ It is a dynamic, evolving biological network
⚠️ Why biomarkers still fail in real life
• Heterogeneity between patients
• Variable kinetics over time
• Lack of standardized thresholds
• Overreliance without clinical context
➡️ Biomarkers alone will NEVER replace clinical reasoning
🔥 Take-home message
The future is not:
👉 “Which biomarker is best?”
The future is:
➡️ Integrated biomarker panels + physiology ....+ AI?
📚 Zheng X. et al. (2026)
Frontiers in Immunology
https://t.co/YXDOXRpFxF
Congratulations to Prof Doruk Ozgediz for the UCSF Exceptional Physician Award! Many Ugandan babies and paediatric surgeons have witnessed his exceptional dedication to surgical (and anaesthesia too!) care. Well deserved! @UCSF_CHESA@ASOU_Official@KidsOperating@stellahalyce
💧 Ultrafiltration in the ICU is not fluid removal…It is hemodynamic stress testing.
🚨 New perspective in critical care:
👉 Ultrafiltration (UF) is a double-edged sword
👉 The relationship with outcomes is U-shaped
📉 Too slow → persistent congestion
📈 Too fast → hypoperfusion & organ injury
🎯 The safe zone is narrow and patient-specific
🧠 We have been thinking about UF incorrectly
❌ “UF intolerance = hypovolemia”
👉 This is wrong
🚀 UF intolerance is MULTIDIMENSIONAL
Defined by failure of 4 physiological axes:
▪️ Vascular refilling
▪️ Cardiac response
▪️ Venous tone / capacitance
▪️ Arteriolar resistance
⚡ Key concept
👉 UF is not just removing fluid
👉 It is testing physiological reserve
🔥 Why patients crash during UF
Not just volume…
🧩 5 clinical endotypes
1. Preload dependence
2. Cardiac dysfunction
3. Vasoplegia (↓ vascular tone)
4. Autonomic dysfunction
5. Low vascular refill
👉 Different mechanism = different treatment
⚠️ Same hypotension ≠ same problem
Giving fluids to all = mistake
Stopping UF always = mistake
🧬 Practical bedside shift
Before UF:
👉 Don’t ask “how much fluid to remove?”
👉 Ask “can this patient tolerate removal?”
🛠️ New tools proposed
▪️ Passive leg lowering (reverse PLR)
▪️ UF challenge (mini fluid removal test)
▪️ Perfusion markers (CRT, PI)
▪️ Multimodal POCUS (LUS + VExUS + cardiac)
🔥 Major clinical implication
👉 UF should be:
✔️ Dynamic
✔️ Personalized
✔️ Preventive (not reactive)
🚀 Paradigm shift
We mastered fluid resuscitation with physiology…
👉 Now it’s time to master fluid removal the same way
⚠️ Take-home
UF is not dialysis mechanics
👉 It is cardiovascular physiology under stress
📚 Melo et al. Critical Care 2026
https://t.co/noOVgs4xIo
@best101bits@Danieobua I don’t even know where to start.
Allow me to borrow a football analogy.
Given how complex football is, I think the Lead Striker should be the one also trained in Defense, having two separate people increases chances of misunderstanding.
🫀 Are we treating numbers… or perfusion?
A compelling perspective from perioperative physiology challenges a core assumption in anesthesia and critical care:
👉 Optimizing MAP or CO does NOT guarantee adequate tissue perfusion.
🔬 Physiological reality: macro ≠ micro
▪️ Tissue perfusion is primarily driven by metabolic demand and local vasoregulation, not just systemic pressure
▪️ Arteriolar vasodilation and capillary recruitment are the real determinants of oxygen delivery
▪️ Increasing MAP via vasopressors may restore pressure but impair flow, especially at the microcirculatory level
⚠️ Anesthesia changes the rules
▪️ ↓ VO₂ (around 25%) alters the DO₂-VO₂ relationship
▪️ Volatile agents → vasodilation + uncoupling of metabolism and perfusion
▪️ Blunted autonomic responses → dependence on external hemodynamic manipulation
➡️ The result: hemodynamic coherence is frequently lost intraoperatively
📉 Why classic strategies fall short
▪️ Goal-directed therapy often targets stroke volume maximization, not perfusion
▪️ Fluid responsiveness ≠ fluid requirement
▪️ Vasopressors may ↑ MAP but ↓ CO and regional oxygenation (brain, kidney)
💡 This explains why large RCTs show heterogeneous or neutral outcomes
🧠 What should we do differently?
👉 Shift the target:
From: MAP, CO, SVR
To:
✔️ Tissue perfusion
✔️ Microcirculatory flow
✔️ Organ oxygenation
But here’s the limitation:
⚠️ We still lack a reliable, practical intraoperative perfusion monitor
🎯 Clinical takeaway
Hemodynamic success should not be defined by “normalized numbers,”
but by restored tissue perfusion.
Until we measure it properly,
we risk treating physiology we assume, not physiology that exists.
📚 Putowski Z et al. (2025).
Journal of Clinical Anesthesia, 107, 112009
https://t.co/YyzfLuBd7k
⚠️ We’ve been explaining calcium in hyperkalemia WRONG for decades.
“Membrane stabilization”?
➡️ Probably not 🤔
🧠 What we were taught:
👉 Calcium restores resting membrane potential (RMP)
👉 That’s why it “stabilizes” the myocardium
Sounds clean.
But… it may be wrong physiology.
🔬 What this study shows:
▪️ Hyperkalemia →
→ ↑ RMP
→ ↓ sodium channel availability
→ severe conduction slowing → QRS widening → sine wave ECG
✔️ Calcium DOES improve ECG
✔️ Calcium DOES restore conduction
❌ But it does NOT restore RMP
⚡ So what is calcium really doing?
👉 It restores conduction velocity, not membrane potential
Mechanism:
▪️ ↑ L-type Ca²⁺ current
▪️ Enables Ca²⁺-dependent propagation
▪️ Bypasses impaired sodium channel conduction
➡️ The heart switches from Na⁺-dependent conduction → Ca²⁺-supported conduction
📉 Key physiological shift
Hyperkalemia:
▪️ Sodium channels ↓
▪️ Conduction fails
Calcium:
▪️ Doesn’t fix the membrane
▪️ Keeps the signal moving anyway
💡 Clinical implication:
👉 Calcium is NOT a “cosmetic ECG fix”
👉 It is a conduction rescue therapy
🎯 Use it when: ▪️ QRS widening
▪️ Conduction delay
▪️ Pre-arrest patterns
⚠️ NOT just for: ▪️ Isolated peaked T waves
🔥 Take-home
We should stop saying:
❌ “Calcium stabilizes the membrane”
And start saying:
✔️ “Calcium restores cardiac conduction during hyperkalemia”
📚 Piktel JS et al. (2024)
Critical Care Medicine
DOI: 10.1097/CCM.0000000000006376
🩺 Arterial line ≠ just a number on the monitor
If you’re only looking at MAP…
you’re missing most of the physiology.
🧠 Invasive BP is a real-time hemodynamic language
Every component tells a different story:
▪️ MAP → organ perfusion
▪️ DAP → vascular tone
▪️ SAP → LV afterload
▪️ Pulse Pressure (PP) → stroke volume surrogate
➡️ It’s not one number.
It’s a dynamic physiological system
⚠️ First rule, often ignored:
👉 If the waveform is wrong → everything is wrong
Before interpreting:
✔️ Check damping
✔️ Perform fast flush test
✔️ Look for:
Rapid upstroke
Dicrotic notch
Smooth diastolic decay
➡️ Bad waveform = bad decisions
📉 MAP alone is NOT enough
We target MAP ≥65 mmHg…
but:
▪️ Duration of hypotension matters
▪️ Individual physiology matters
▪️ CVP matters
👉 Think instead:
🎯 Perfusion pressure = MAP − CVP (MPP)
➡️ A “normal MAP” can still mean hypoperfusion
🔥 DAP = your vasopressor trigger
Low DAP = low vascular tone
▪️ Septic shock → ↓ DAP
▪️ Early signal before MAP collapses
👉 Use it to:
✔️ Start norepinephrine earlier
✔️ Avoid delayed vasopressor therapy
➡️ It’s one of the most underused variables in ICU
⚡ Pulse Pressure = hidden CO monitor
PP reflects:
▪️ Stroke volume
▪️ Arterial stiffness
👉 Dynamic changes = key:
✔️ PLR
✔️ Fluid challenge
✔️ Ventilator cycles (PPV)
➡️ You can track CO trends without a CO monitor
🧬 Next-level physiology (very underrated):
New indices:
▪️ DSI = HR / DAP
→ identifies vasoplegia early
▪️ VNERi = DAP / (HR × NE dose)
→ detects norepinephrine resistance
👉 These may define who needs vasopressin early
💡 Mindset shift
Don’t ask:
❌ “What’s the MAP?”
Ask:
✔️ “What is the physiology behind this waveform?”
🧠 Take-home
Arterial line monitoring is not passive.
It’s:
▪️ Diagnostic
▪️ Therapeutic
▪️ Predictive
➡️ If you read it correctly…
it becomes a precision resuscitation tool
📚 Bertrand M et al. (2025)Annals of Intensive Care
DOI: 10.1186/s13613-025-01608-y
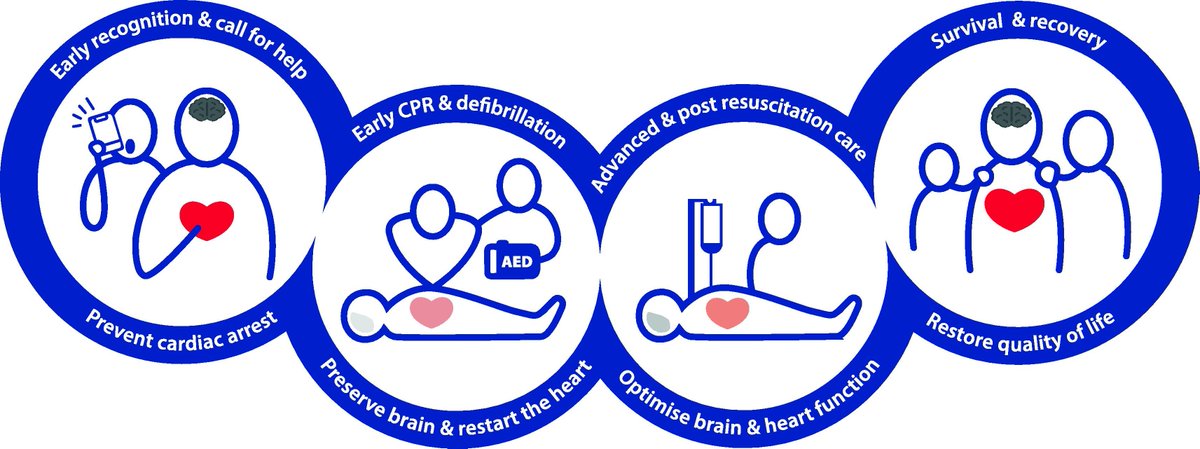
The 2025 European Resuscitation Council Guidelines have been released
All 11 plus the executive summary included below
CCR Journal Watch
https://t.co/Sp06oA6IDG
🧩 Part 3 – Why you usually can’t move one curve without the other
1️⃣
So far, we’ve treated the cardiac and venous return curves as two lines that meet.
In theory, you can move one without the other – and sometimes that’s true.
But in physiology, they almost always move together – because they share the same inlet.