I’ve looked at this #EHA2026 slide 100x but it still always makes me pause.
Unexpected early relapses so scary for patients with myeloma, and historically post-PD OS in FHRMM ≤ 2 years no matter what we do.
Here, off-the-shelf Tx boosted 3-yr PFS from 0% to 77%. Giving these pts a fighting chance for deep & durable remissions 🥹
Pictures worth 1000 words - excellent 🇩🇰 #MMsm work in @AjHematology!
ABCD study of prophylactic toci and analysis of primary IVIG PPx with BCMA bsAbs in myeloma.
Answer clear as day: both PPx toci and PPx IVIG are essential safety interventions 💪🏻 We need to work on ⬇️ cost!
The main change for this cycle: "Ciltacabtagene autoleucel or the combination of teclistamab and daratumumab are preferred options at first relapse in eligible patients who have not previously received B-cell maturation antigen (BCMA) directed therapy. Teclistimatab plus daratumumab is not recommended for patients who are refractory."
More is sure to come with updates from ASCO 2026.
You can see the quarterly updates here! https://t.co/0gEvNrYM3G
Thank you to the Nason Hollingsworth and Argyros families for making Jay Seq a reality : You have truly changed lives for patients with myeloma. All led by our rockstar Dr Johnathan Keats!
High risk smoldering myeloma.
18 months later.
FDA approved
EU approved
NCCN Level 1
Despite a few experts throwing cold water, daratumumab is now widely used for high risk smoldering myeloma in the US. Makes sense because it works. And clinicians are not keen on waiting till renal failure or lytic bone lesions to start therapy. Our patients want to prevent them in the first place. That’s the whole idea.
❓️ What does "transplant-ineligible" even mean anymore?
@RahulBanerjeeMD, of @fredhutch, reflects on the recent Dara-VRd approval for transplant-ineligible, newly diagnosed #myeloma and how transplant-based trials no longer match real-world care.
📖 https://t.co/JL3Cgdemru
At the @Myeloma_Society CURE Summit. We are talking about defining cure in myeloma and designing trials to achieve a cure
Thanks to @NikhilMunshiMD@VincentRK@myelomaMD and others for their vision to get us to this point and lay the path forward for us as a field #mmsm
Reassessing the Duration of Induction Therapy for Newly Diagnosed, Transplant-Eligible Myeloma Patients in the Context of Quadruple CD38 Monoclonal Antibody-Based Regimens: Is 24 Weeks Optimal?
https://t.co/4rp1jXt1r5
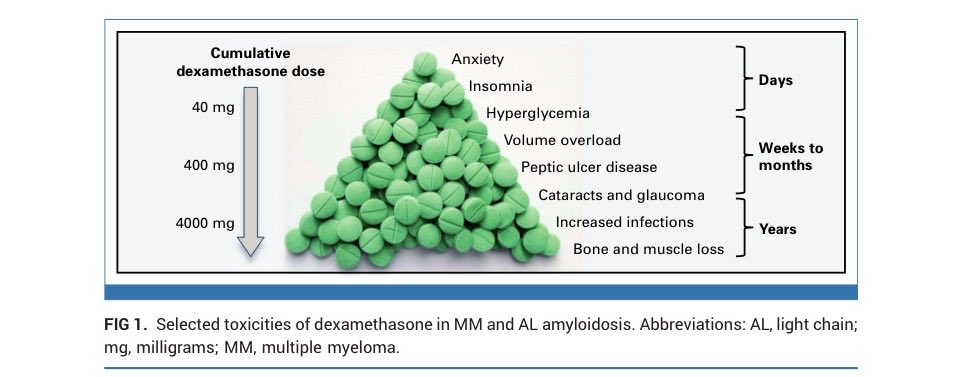
Past, Present, and Future of Dexamethasone in Multiple Myeloma and AL Amyloidosis | Journal of Clinical Oncology #mmsm@JCO_ASCO@RahulBanerjeeMD@Bethfaiman@vsanchorawala@jmikhaelmd
Nice article on the role of steroids in myeloma and AL amyloidosis. I think this likely apply to other medications were we may need to dose reduce or treat for a fixed duration of time
➡️https://t.co/J7iQCEtWKL
We have now 3 CT with T-cell redirecting therapy vs. Triples in 1-3 prior LOT in MM with OS superiority. I don't consider acceptable to start randomized trials with DPd/Kd/EPd/etc control when we have proven superior "established therapy with clinical benefit". #mmsm
This slide explains the current strategy for smoldering myeloma trials. I use it as an example. It is useful to study this for anyone interested in a career in strategic clinical trials.
What do we do if we need to test multiple strategies to solve a clinical problem, when each step of each strategy takes more than a decade to accomplish? This is the situation we face in SMM. And here is how we are approaching it.
In SMM we have 3 key strategies to test. Each is an important question to be addressed in our strategy to improve outcomes for patients. We are tackling this problem by testing all of these 3 key strategies in parallel. We will be happy if any one of these succeeds, or whether all 3 are successful.
The 3 strategies tackle 3 problems, all of which are important and time is of the essence.
Question 1) Does early therapy improve outcome in smoldering myeloma, and if it does how do we make it available to patients worldwide? To address this in a manner that actually helps patients we need to first prove one drug is better than nothing. No regulator will approve early therapy if you test Dara-VRd vs observation. You won’t know which drug is essential and which is not. You have to prove 1 is better than 0, before you get to 2 is better than 1, and do on. As we did with active myeloma. These are necessary trials. Without this step we won’t get regulatory approval for anything. And without regulatory approval even if early therapy is useful, few patients outside the US will have access. These are also incredibly difficult trials because SMM is much less frequently diagnosed than active MM, and because endpoints take much longer.
Question 2) If early therapy is indeed helpful, will patients have better outcomes and live longer with monotherapy or with myeloma-like combination therapy? Ideally you would like to do this after you find out that monotherapy is helpful, but time is of the essence and many patients want to test early intervention. So shortly after the first monotherapy trial shows promise, we embarked on these trials to test what is the optimal way to approach early therapy. Two phase IIIs have been done: IsaRd vs Rd and DaraRd vs Rd. One has completed accrual and one is almost done with accrual. Results will take time, but far sooner than if we were just starting to design such trials.
This is the advantage of anticipating results and designing successor trials. We have done this over and over again in myeloma successfully.
Question 3) Can intervention used early in the SMM stage actually result in a cure? In other words, instead of just delaying myeloma or improving overall survival, can early intervention deliver an actual cure! We don’t need early intervention to be curative; delaying myeloma, delaying or preventing need for myeloma like therapy, or improving overall survival is sufficient. But cure will be surely great and the question of whether and if so which therapy will be curative is important. Again we have embarked on trials to address this question in parallel. Trials targeting cure as a goal like Cesar and Ascent have been done. And more such trials are on their way.
When we think about solving a clinical problem sometimes we have to test multiple key questions. Having a clear thoughtful vision, identifying the key questions and strategy on how to address them, having a world view rather than views centered on your own country or situation, and having international collaborations to address them is important.
We are fortunate in the myeloma field that as a team we are able to work with colleagues, companies, patients, foundations, around the world to address them. SMM is a good example, but the field is full of them.
I hope this is useful for those trying to develop a career in conducting meaningful clinical trials. The ultimate reward is when efforts lead to a practice change that helps patients worldwide
@mvmateos@SagarLonialMD@thanosdimop@Mohty_EBMT@End_myeloma@szusmani
Thanks @VuMedi for letting me get onto even bigger soapbox re: importance of IgRT (IVIG/SCIG) with bsAbs in myeloma #MMsm.
BsAbs are like no other drug past or present re: high infection risk...
Enough data to start IVIG during Cycle 1. Don't wait for infection or death!
Results of the MajesTEC-3 for #myeloma just published: https://t.co/c4wuBVITy3 Pending approval in earlier lines, this will change the paradigm of using bispecific antibodies in myeloma. #mmsm
All the FDA approvals for relapsed myeloma in one slide.
20 drugs in 20 years is possible only by collaboration among industry, disease experts, patients, agencies, and foundations. Myeloma is a role model. Thats why we have mode than quadrupled the expected overall survival. #ASH25
#ASH25 US Multiple Myeloma Immunotherapy consortium
We presented 14 orals, 8 posters at ASH!
Now with 25+ sites
Could never have imagined this success when Dr Hansen, Patel and I co-founded this 4+ years ago.
Incredible collaborative effort!! A lot of work goes into this.
#ASH25@End_myeloma moving the field forward with another MASTERful presentation (pun only partially intended).
While we’ve often defined FHRMM as 18 months after induction, times are a-changin’ with quads.
36 mo is the new 18 mo: if relapse ≤ then, go to bsAbs or CAR-T!
#ASH25 saying it louder for everyone in the back!
If you are starting a bsAb in #MMsm (especially BCMA), don’t wait for patient to die or IgG to drop. Start IgRT now!
Newest case in point: excellent IFM 2021-01 trial. Only 14% Gr3+ infxns despite older pts & CD38 pair!