Salbutamol nebulization and High lactate.
This classic presentation is due to Salbutamol-Induced Lactic Acidosis (SILA), a well-documented Type B lactic acidosis.
*High or frequent doses of β₂-agonists trigger a sequence of metabolic changes that completely mimic a septic picture.
●Here is exactly why this happens:
1. Tremor:
Salbutamol stimulates β₂-adrenergic receptors in skeletal muscle, resulting in increased cyclic AMP (cAMP) production.
This heightened adrenergic state leads to increased glycogenolysis (the breakdown of glycogen into glucose) and subsequent muscle tremors.
2. Tachycardia:
High circulating levels of salbutamol start to stimulate β₁-adrenergic receptors (the primary receptors in the heart) in addition to β₂-receptors, directly causing a rapid heart rate (palpitations) and a drop in diastolic blood pressure.
3. High Lactate:
Salbutamol-induced intracellular cAMP accumulation aggressively stimulates both glycolysis (the breakdown of glucose) and lipolysis (the breakdown of fats into free fatty acids).
The massive amount of glucose being broken down creates excess pyruvate.
Simultaneously, the free fatty acids inhibit the enzyme that converts pyruvate into acetyl-CoA.
Left with nowhere else to go, this pyruvate is rapidly converted by the body into lactate.
4. Worsening the Vicious Cycle:
Co-administered steroids (like hydrocortisone or dexamethasone) increase β₂-receptor sensitivity, which further heightens lactate production.
The rising lactate creates a metabolic acidosis, making the patient breathe faster (tachypnea), which can be falsely interpreted as a worsening respiratory infection.
■The Takeaway...
When a patient receiving frequent salbutamol nebulization develops a high lactate, tachycardia, and tremor, SILA should be considered before presuming worsening sepsis.
Unlike sepsis-induced Type A lactic acidosis (which results from poor tissue perfusion), Type B lactic acidosis resolves rapidly when the offending β₂-agonist is reduced or discontinued.
https://t.co/gsFj3Or5di
The Frank–Starling law, described by Otto Frank and Ernest Starling, explains how the heart adjusts its output. It states that:
"as more blood fills the ventricles (↑ preload), the heart pumps more forcefully, increasing stroke volume "
In the graph:
🔵 Normal curve: Stroke volume increases with preload, then levels off.
🟢 Improved function: With better contractility or lower afterload, the heart pumps more efficiently.
🔴 Poor function: In heart failure (↓ contractility or ↑ afterload), stroke volume increases slightly, then drops ("falling off").
🔵 Giving fluids only helps in the preload-dependent zone. Beyond that, it may worsen function.
🔵 The lowest curve shows cardiogenic shock, where extra preload barely helps.
Clinical use: Helps guide fluid therapy and avoid overload in heart failure.
Slowing aging is not theoretical. In humans, calorie restriction measurably slows biological aging pace by ~2–3% over 2 years
Link here: https://t.co/Eg8wBzhDpQ
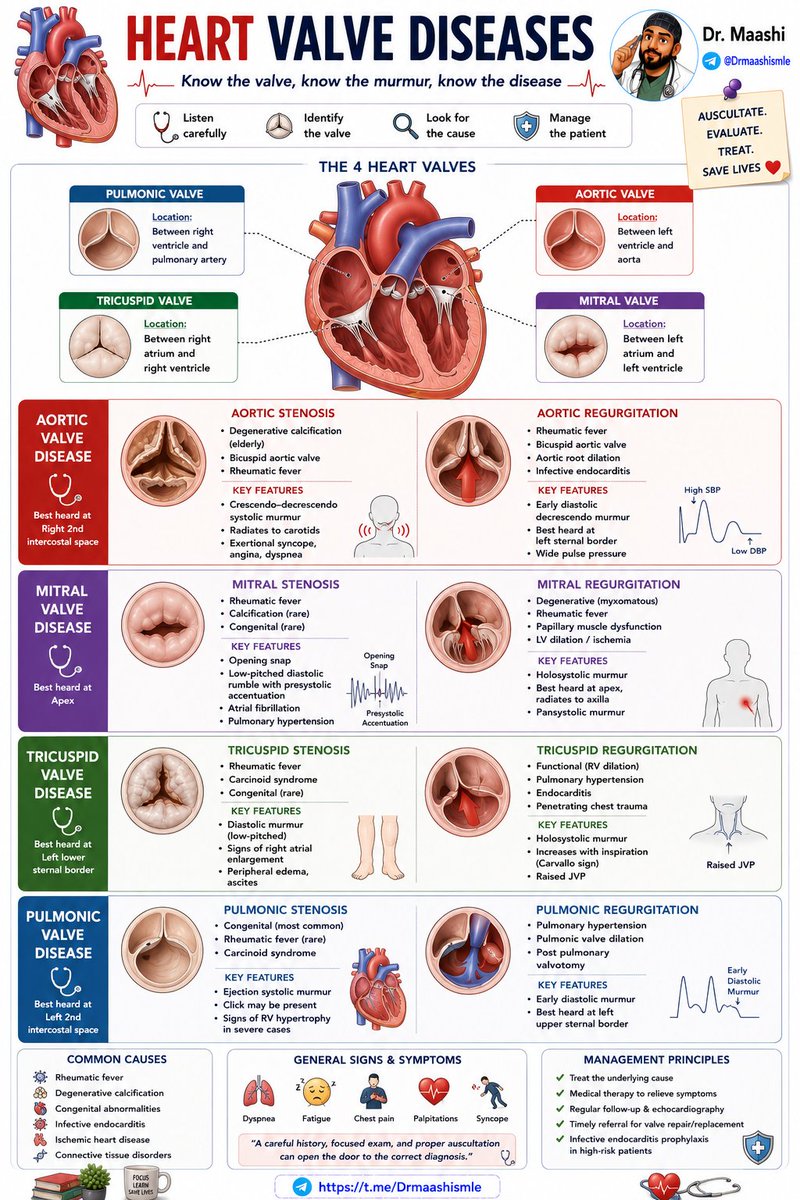
Heart valve disease is more than just a murmur 👀
📌 Aortic stenosis → Syncope, angina, dyspnea
📌 Mitral stenosis → Opening snap + atrial fibrillation
📌 Mitral regurgitation → Murmur radiating to the axilla
📌 Aortic regurgitation → Wide pulse pressure
Know the valve.
Know the murmur.
Know the diagnosis. ❤️🩺
A high-yield review of valvular heart disease with anatomy, murmurs, clinical clues, and exam pearls.
https://t.co/1dSdJ0pv1C