So $ABVX went from ~$180 after hours to ~$69 on the slide below, which people have (misguidedly IMO) interpreted as a cancer risk in the high dose arm.
This looks very much like noise - 2 cases (one each, a rate of 0.5%) of the 2 most common cancers in the world (breast and prostate). Zero cases in the low dose arm. NMSC is a throwaway side note and almost always age related - as they noted they *were* in this case. The only thing to adjudicate is the prostate and breast cases.
They also noted ZERO cases in the long term extension study from phase 2, which consisted of well over 100 patients and has had some patients on drug for 7+ years, ALL of them on drug for >2 years.
2 cases (again, 1 each) of the 2 most common cancers in the world among all those patients (P2+P3) over all those years. This is noise.
Let's say you *don't* think this is noise for the high dose...
Well, then it's a good thing that the low dose showed zero malignancy signal vs placebo and *still* came in with efficacy vastly above the market's expectations (39% delta vs 40% for the high dose).
The low dose with 39.3% delta and no cancer signal is right there with the (previously) highest reported efficacy drug, Rinvoq...Except, Rinvoq has a black box warning that has *5* bullet points:
-Serious infections "leading to hospitalization or death"
-Higher rate of all cause mortality "including sudden cardiovascular death"
-MALIGNANCIES "including lymphomas and lung cancers"
-Higher rate of MACE (including heart attacks and strokes)
-Thrombosis (including pulmonary embolism)
So, let's say you do think this gets a black box warning for malignancy risk (even despite all the notes above, and the fact that the low dose had zero cases of non-NMSC malignancy and was balanced with placebo on NMSC)...
...then you are looking at a WORST CASE scenario of 1 bullet on a black box warning versus *5* for Rinvoq (and the other JAK inhibitors).
The 2nd highest clinical remission delta for a non black box warning drug ever is...Entyvio at 26%....
So you have 2 JAKi with 5 black box warning "points" and remission deltas of 39.8% (Rinvoq) and 30% (Xeljanz).
Again, WORST case, $ABVX gets 1 black box warning "point" despite all the evidence that this is just noise and had 39.3% and 40.3% remission delta.
Want something without a black box? You're looking at 20-26% delta. And again, that's *if* this is actually something the FDA doesn't think is noise. You've got the 25mg dose with literally zero signal versus placebo and 7+year P2 dataset saying zero signal as well with many of those patients having been on higher than 25 mg doses.
At $70 AH this is a $6B company? Absurd from my perspective. At worst this is the most efficacious drug in the industry with a black box warning 1/5th as bad as the JAKis that do big numbers in this disease at WORST.
my response to an unhinged take:
first, median overall survival doesn't count fat tails. SOME patients will the lottery and get 3 or 5 more years of life. wish i still had my dad who died of cardiovascular disease!
next, this is how progress happens. i made a post a few weeks ago about how mOS for multiple myeloma has gone from something like 6 months to 5 years over the last 20 years. thats amazing progress. the progress compounds. cheer on progress--it's not hard. our children and their children's children will still get cancer, we owe it to them to give them the best outcomes.
finally, no one is trying to make half a medicine. when you make a molecule you're giving it your all. you don't dial it down and say 'well, 6 months is enough' as if anyone sets this kind of goal. (it's not even scientifically possible). you make it and see what you get. somewhat invariably, there is no 'cure' lurking that you missed. you hit one pathway, then another, and then another, and then you get a real long-term outcome shift. it's the same story in every tumor type (excluding a few like CML where pharma hit it out of the park). if a 'cure' is so easy, start a drug company and do it yourself!
FYI drug = daraxonrasib.
Very promising early clinical signals in pancreas cancer. Ongoing/future studies will be important in establishing efficacy & characterizing toxicity (& how to best manage).
Recently I was at a dinner with other investors and we were lamenting pitches where there’s a “fast talker”. As a presenter, it’s always good to check yourself to determine if you’re talking at a speed that allows your audience to do several things at once: 1) hear and comprehend what you’re saying; 2) take notes; 3) look at the slide to correlate what you’re saying with the figures there; 4) formulate and ask questions. The speed at which you can transmit information as a person intimately familiar with your slides / data is going to be much faster than someone new to the story can absorb it. The goal should not be to transmit as much information as possible by talking at maximum speed. There is no way to tell investors everything on a one hour call; focus on presenting a cogent argument with enough data to be persuasive, but without so much detail that it’s overwhelming. Make sure there’s time for questions along the way. Note that it’s more important to hit every key point high-level, than it is to go into great detail about certain points (e.g., don’t completely neglect to mention IP, competition, etc., simply to add one more data slide).
Another habit to avoid along these lines – talking (or pontificating) for a long period of time on a single slide, particularly when there are other slides in the deck that actually make each of your points. Many people are visual learners, so make full use of the slides you’ve prepared.
the only viable US biotechs going fwd are:
i) novel platform tech (better way to find target, have better selectivity, or super power efficacy in a particular modality)
OR
ii) clinical team that can "king-make" a best in class mlc from China or an AI shop (ie uniquely experienced team for a particular disease indication that has specific expertise for shepherding programs through difficult to execute indications eg rare disease, respiratory, etc)
every co in the middle (potential best in class mlc w/o differentiated clinical team, me-better approaches, and even novel targets without unique clinical strategy) is on the clock
🚨 JUST IN: Eli Lilly ($LLY) releases blockbuster results on it’s oral GLP-1
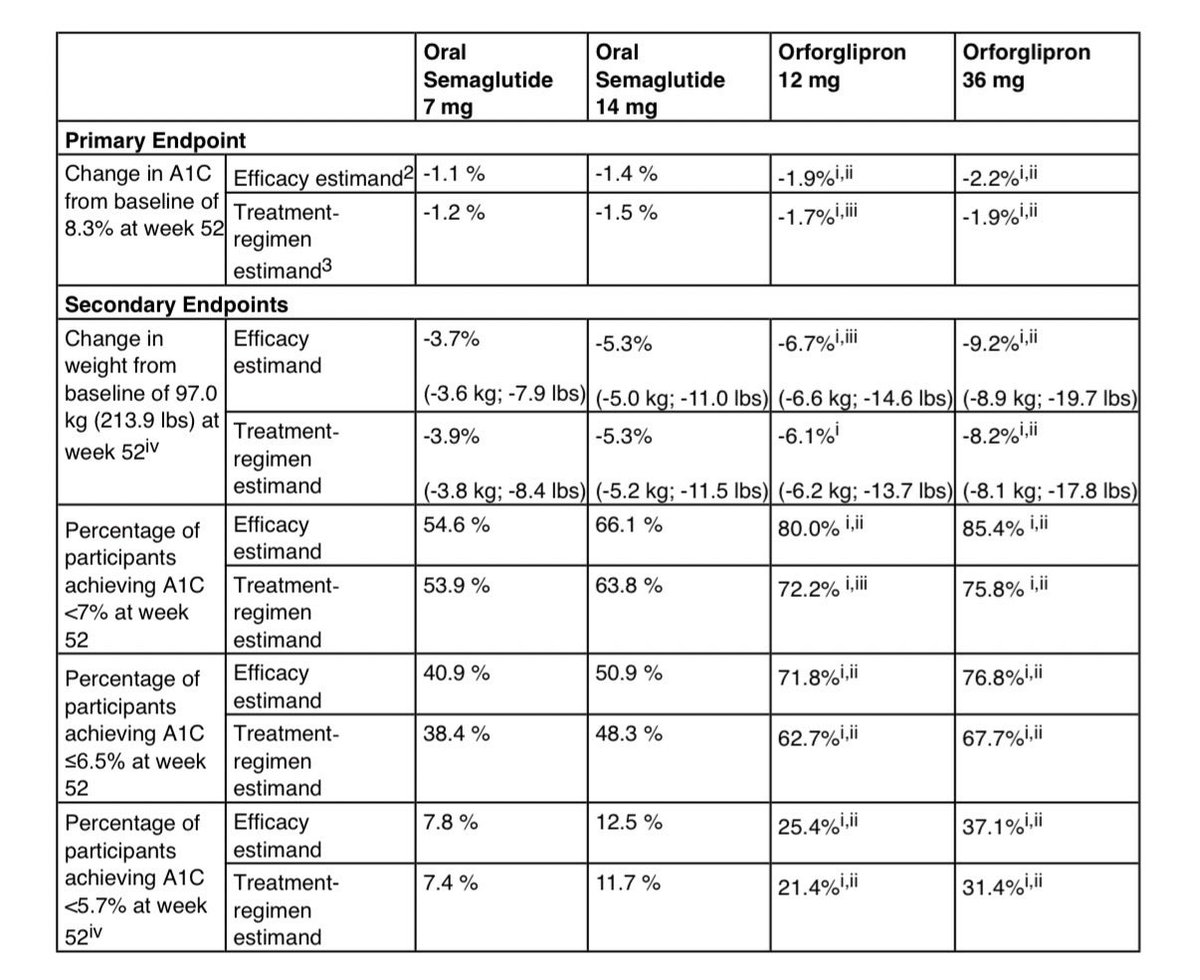
Eli Lilly just posted head-to-head data showing its oral GLP-1, orforglipron, beat oral semaglutide across blood sugar and weight loss in a 52-week Phase 3 trial.
Top-line trial details
- ~1,700 adults with type 2 diabetes
- Head-to-head vs oral semaglutide 7 mg and 14 mg
- Doses tested: orforglipron 12 mg and 36 mg
Primary endpoint: A1C reduction
- Orforglipron 36 mg: −2.2% A1C
- Oral semaglutide 14 mg: −1.4% A1C
Weight loss
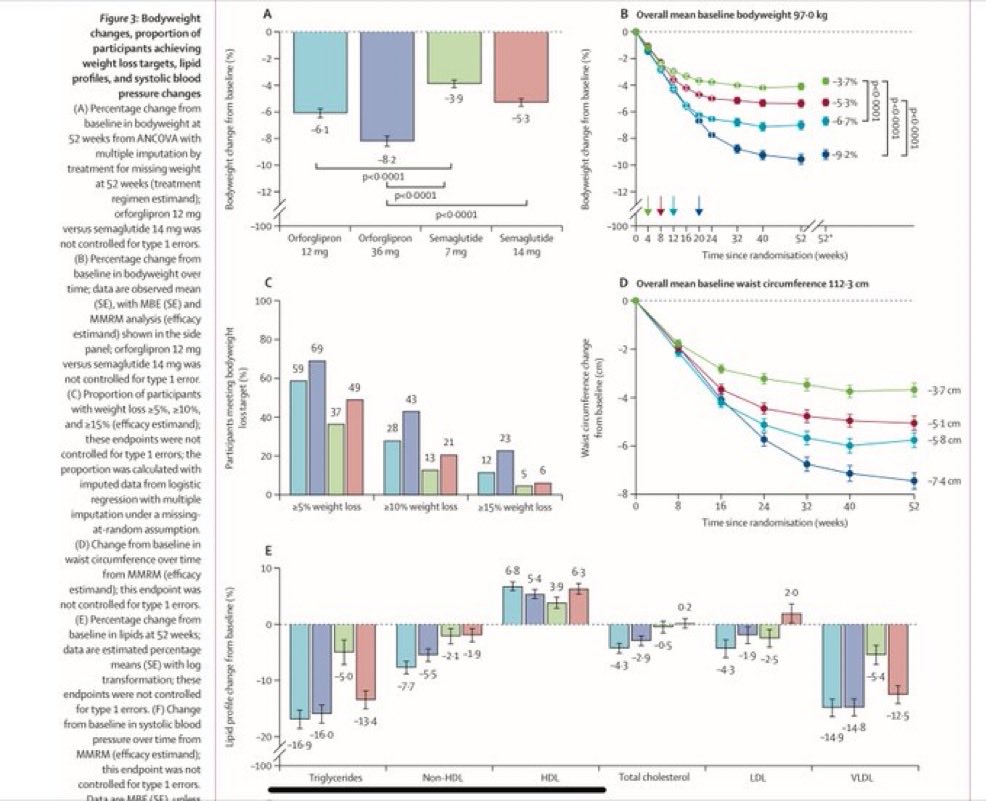
- Orforglipron 36 mg: −19.7 lbs (−9.2%)
- Oral semaglutide 14 mg: −11.0 lbs (−5.3%)
- Roughly 7.3% greater relative weight loss
That puts Lilly’s oral small molecule into weight loss territory approaching injectables 🤯
Orforglipron also improved:
- Non-HDL cholesterol
- HDL cholesterol
- LDL cholesterol
- VLDL cholesterol
- Total cholesterol
- Systolic blood pressure
- Triglycerides
Importantly, orforglipron did have HIGHER Adverse Events like nausea, diarrhea, vomiting, dyspepsia, decreased appetite, leading to more people dropping off…
Discontinuation due to AEs:
- Orforglipron 36 mg: 9.7%
- Oral semaglutide 14 mg: 4.9%
But, good news is that it’s a daily tablet with no food or water restrictions that greatly outperforms $NVO’s Wegovy pill.
Another big win for Lilly.
Someone shared this on LinkedIn, great comment. "The FDA approves drugs based on clinical meaningfulness. Payers reimburse drugs based on economic value and real-world applicability".
@zhaoweiasu Still in the early innings. Agreed, Phase 2 BROADEN2 study (n = 200) with the placebo arm will be more representative.
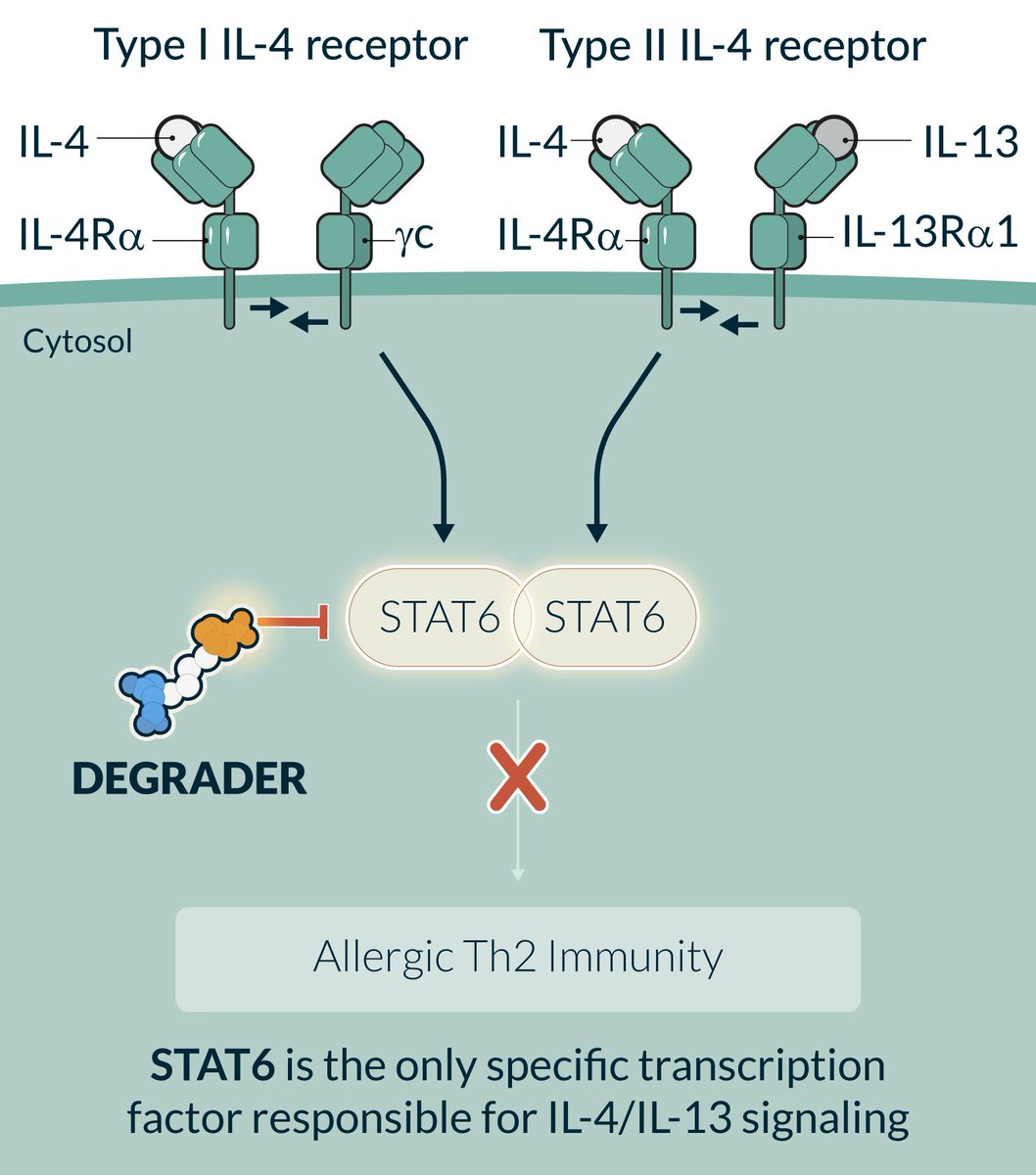
STAT6 is the only specific transcription factor responsible for IL-4/IL-13 signaling. A oral degrader for STAT6 makes sense from a chronic use standpoint.
@shelbynewsad slightly related, but a big fan of Solarea Bio's microbe-based medical food. Hip fracture risk for women is insane due to osteopenia. Nicely designed clinical study.
Bōndia slowed the rate of bone density loss by 85%. https://t.co/ErDkI9Hr5c
The outsourcing of data generation via CRO is integral. At the same time, "Unemployed Americans with 4-year college degrees now make up a record 25.3% of total unemployment. This comes as over 1.9 million workers aged 25+ with at least a bachelor’s degree are now unemployed."
Atlas Venture 2025 Year In Review https://t.co/qoUKkkAeAS
Been a tough year to pin down as we went from bearish spring to bullish yea end…
Listening at 1.25x+ speed is definitely recommended, and moves through the nearly 50-minute presentation slightly faster.